
philhealth claim form can be completed online without any problem. Simply open FormsPal PDF tool to complete the task right away. The editor is continually improved by our team, acquiring new awesome features and turning out to be greater. If you're looking to get going, here is what it takes:
Step 1: Press the "Get Form" button at the top of this page to open our editor.
Step 2: The editor offers you the capability to change almost all PDF documents in various ways. Transform it by writing customized text, correct original content, and place in a signature - all at your convenience!
This PDF requires particular details to be entered, so be sure you take the time to enter what is expected:
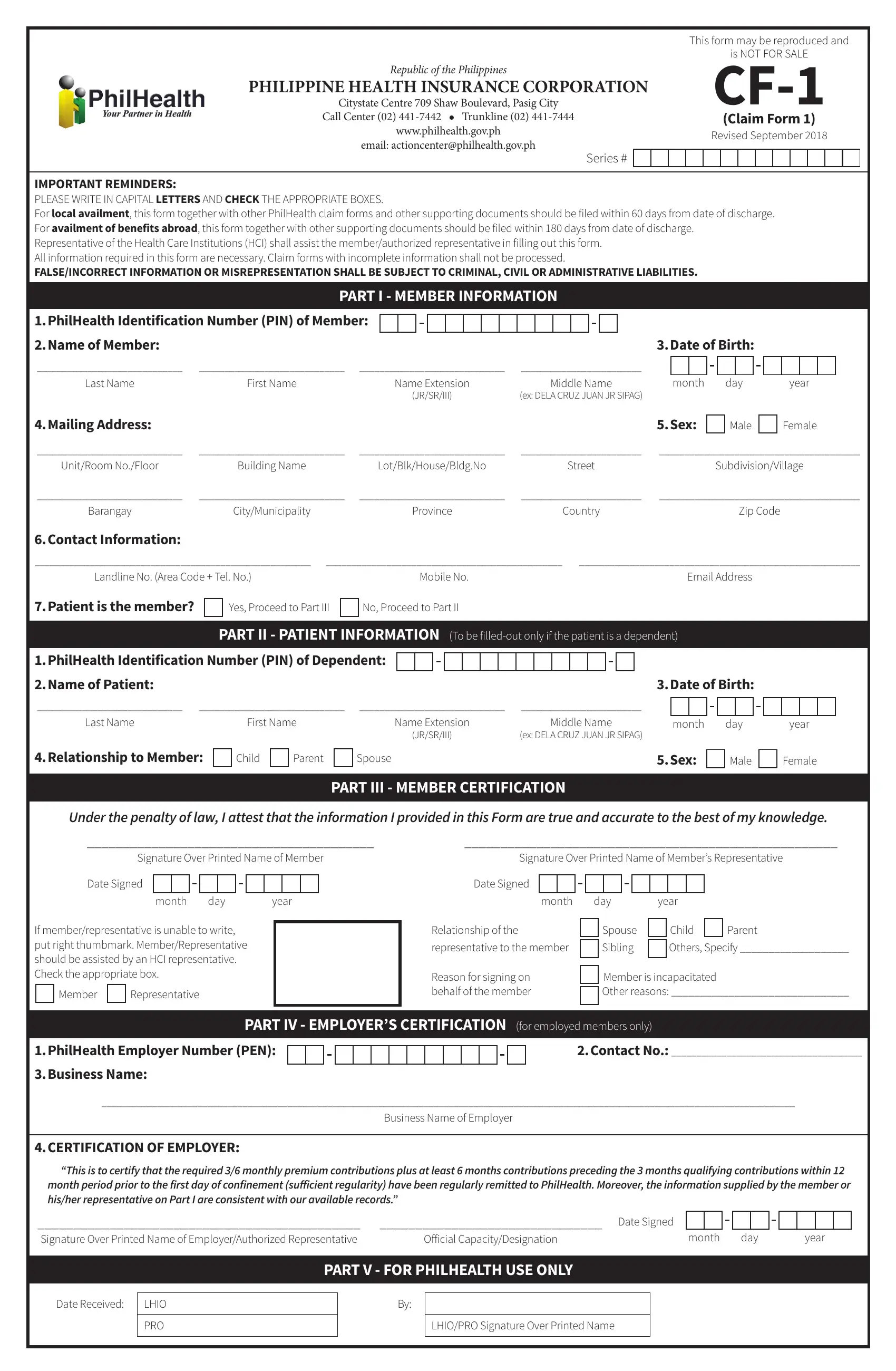
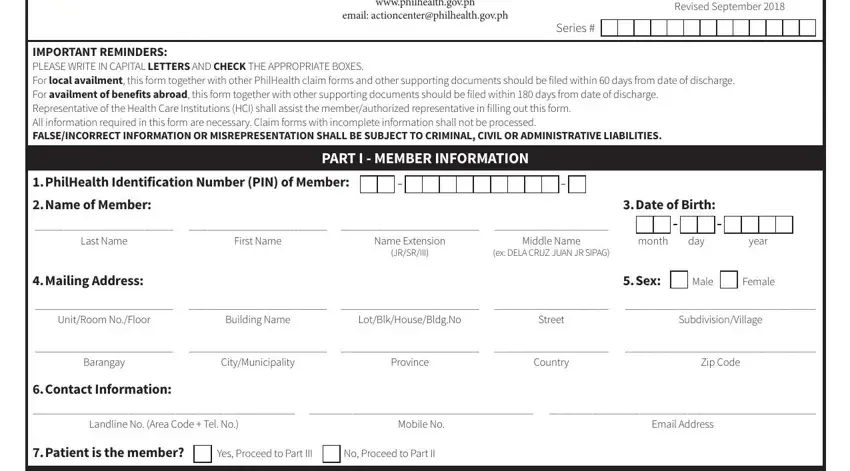
1. The philhealth claim form needs specific information to be entered. Make certain the following blank fields are filled out:
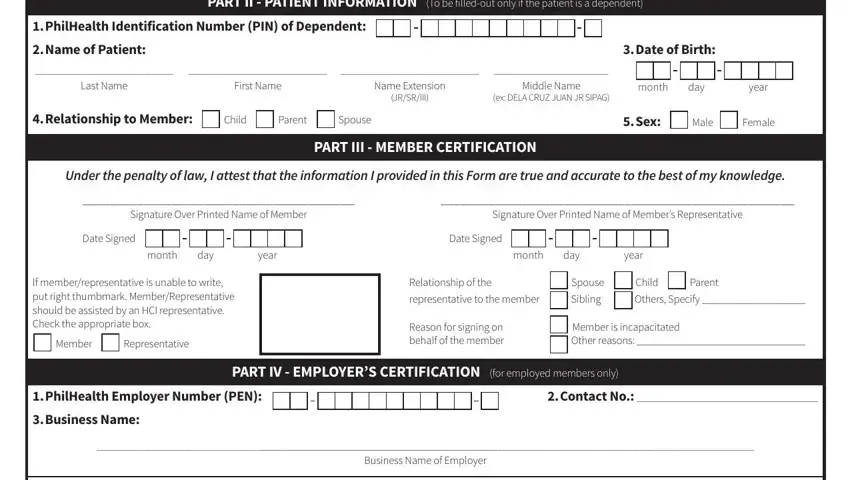
2. Once your current task is complete, take the next step – fill out all of these fields - PART II PATIENT INFORMATION To be, PhilHealth Identification Number, Name of Patient, Date of Birth, Last Name, First Name, Name Extension, JRSRIII, Middle Name, ex DELA CRUZ JUAN JR SIPAG, month day year, Relationship to Member Child, Sex Male Female, PART III MEMBER CERTIFICATION, and Under the penalty of law I attest with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This third stage is hassle-free - fill out all of the blanks in month period prior to the first, Signature Over Printed Name of, Date Signed, Official CapacityDesignation, month day year, PART V FOR PHILHEALTH USE ONLY, Date Received, LHIO, PRO, and LHIOPRO Signature Over Printed Name to conclude this part.

When it comes to Official CapacityDesignation and PRO, be certain you don't make any errors in this current part. Those two could be the most significant fields in this PDF.
Step 3: When you have reread the information you filled in, press "Done" to finalize your FormsPal process. Make a 7-day free trial account at FormsPal and get immediate access to philhealth claim form - downloadable, emailable, and editable in your FormsPal account page. FormsPal is focused on the confidentiality of our users; we always make sure that all personal data entered into our system continues to be secure.