Form Phs 7044 is an important form that business owners and individuals need to be familiar with. This form is used to report income, expenses, and other information related to a business or enterprise. It's important to understand the purpose of Form Phs 7044 in order to correctly complete it and file it with the appropriate government agency. By understanding the requirements of this form, you can ensure that your business is in compliance with tax laws.
| Question | Answer |
|---|---|
| Form Name | Form Phs 7044 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CC26, phs 7044 1 fillable, phs 7044 1, seq |
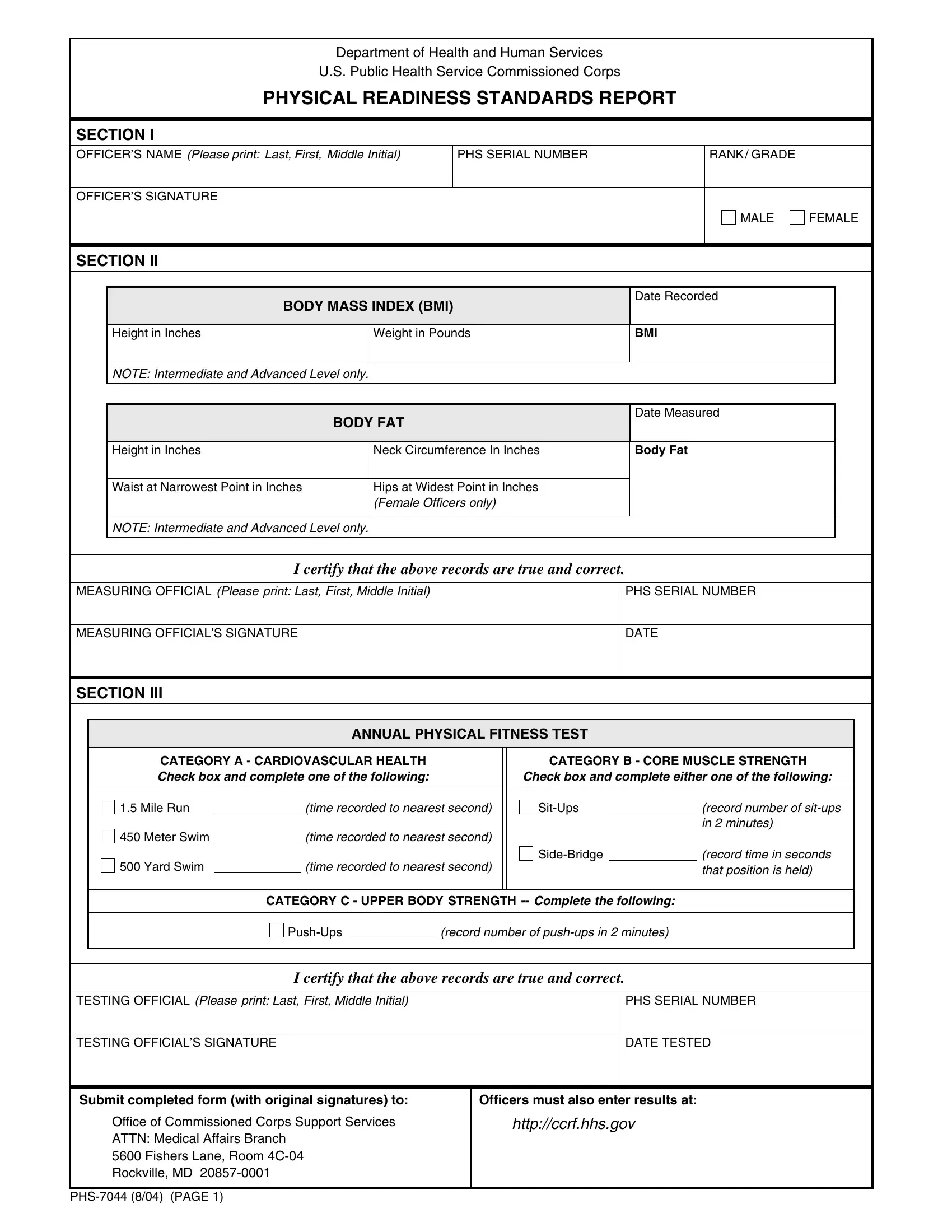
Department of Health and Human Services
U.S. Public Health Service Commissioned Corps
PHYSICAL READINESS STANDARDS REPORT
SECTION I
OFFICER’S NAME (Please print: Last, First, Middle Initial) |
|
PHS SERIAL NUMBER |
|
RANK / GRADE |
|
|
|||
|
|
|
|
|
|
|
|
|
|
OFFICER’S SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MALE |
FEMALE |
|
|
|
|
|
|
|
|
|
|
|
SECTION II |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BODY MASS INDEX (BMI) |
|
Date Recorded |
|
|
||||
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Height in Inches |
|
Weight in Pounds |
BMI |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
NOTE: Intermediate and Advanced Level only. |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
BODY FAT |
|
Date Measured |
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
Height in Inches |
|
Neck Circumference In Inches |
Body Fat |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
Waist at Narrowest Point in Inches |
|
Hips at Widest Point in Inches |
|
|
|
|
||
|
|
|
(Female Officers only) |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
NOTE: Intermediate and Advanced Level only.
I certify that the above records are true and correct.
MEASURING OFFICIAL (Please print: Last, First, Middle Initial) |
PHS SERIAL NUMBER |
|
|
MEASURING OFFICIAL’S SIGNATURE |
DATE |
|
|
SECTION III
ANNUAL PHYSICAL FITNESS TEST
CATEGORY A - CARDIOVASCULAR HEALTH
Check box and complete one of the following:
1.5 Mile Run |
|
(time recorded to nearest second) |
450 Meter Swim |
|
(time recorded to nearest second) |
500 Yard Swim |
|
(time recorded to nearest second) |
CATEGORY B - CORE MUSCLE STRENGTH Check box and complete either one of the following:
|
(record number of |
|
|
|
in 2 minutes) |
|
(record time in seconds |
|
|
|
that position is held) |
CATEGORY C - UPPER BODY STRENGTH
|
(record number of |
I certify that the above records are true and correct.
TESTING OFFICIAL (Please print: Last, First, Middle Initial)
PHS SERIAL NUMBER
TESTING OFFICIAL’S SIGNATURE
DATE TESTED
Submit completed form (with original signatures) to:
Office of Commissioned Corps Support Services
ATTN: Medical Affairs Branch
5600 Fishers Lane, Room
Rockville, MD
Officers must also enter results at:
http://ccrf.hhs.gov
INSTRUCTIONS TO
PHYSICAL READINESS STANDARDS REPORT,
FORM
All
The officer being measured/tested must complete and sign Section I of this report. The Measuring Official/Testing Official must complete and certify Sections II and III. The officer must submit the completed report (with original signatures) to the address at the bottom of the report and enter results at http://ccrf.hhs.gov .
PRIVACY ACT STATEMENT
AUTHORITY: 42 U.S.C. 202 et seq, E.O. 9397, and Subchapter CC26.1, INSTRUCTION 8, of the Commissioned Corps Personnel Manual.
PRINCIPAL PURPOSE(S): To obtain data necessary for determining officer’s level of Force Readiness.
ROUTINE USE(S): None.
DISCLOSURE: Voluntary; however, refusal to submit information will affect the determination of officer’s level of Force Readiness and may impact the officer’s promotion potential. Officer’s PHS serial number is required for identification purposes.
SYSTEM NOTICE FOR RECORDS SYSTEM: The information provided on this report will become part of record system
INSTRUCTIONS |