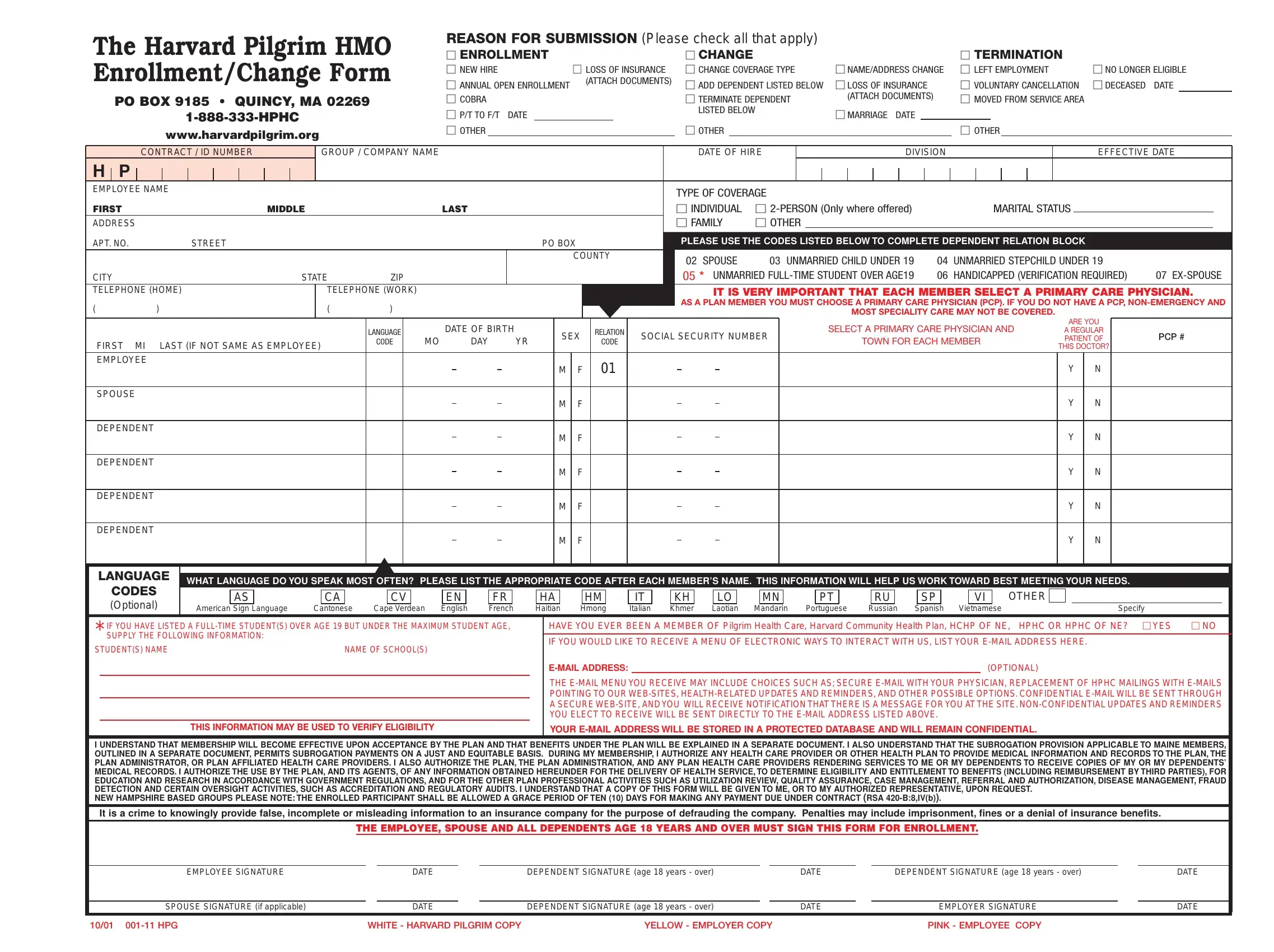
The Pilgrim Enrollment Form serves a crucial purpose in the employment and healthcare sectors, particularly for those associated with Harvard Pilgrim Health Care. It is designed to process various requests such as enrollment in health insurance, changes to an existing policy (like coverage type adjustments, name or address modifications), or the termination of insurance coverage. This form encompasses a wide range of situations including new hires (necessitating the attachment of relevant documents), changes due to marital status, employment status changes (such as moving from part-time to full-time employment or vice versa), the addition or loss of dependents, and voluntary or involuntary termination of coverage. Additionally, it is a channel through which individuals can opt into electronic communication for updates and health-related information, ensuring a more integrated approach to healthcare service delivery. Critical personal info such as the selection of a primary care physician (PCP), marital status, and information on dependents is collected to tailor healthcare services to individual needs. Moreover, it addresses specific scenarios like coverage for full-time students over age 19, and outlines the importance of honesty in providing information to avoid fraud. The form emphasizes the importance of selecting a primary care physician — a decision that could significantly impact the coverage of non-emergency and specialty care services. Ultimately, this document is a comprehensive tool for managing healthcare benefits, adapting to life changes, and ensuring that the healthcare needs of employees and their families are met efficiently.
| Question | Answer |
|---|---|
| Form Name | Pilgrim Enrollment Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | pilgrim change form, harvard pilgrim prior authorization form, harvard pilgrim medicare prior authorization form, hmo enrollment form |
The Harvard Pilgrim HMO |
REASON FOR SUBMISSION (Please check all that apply) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
ENROLLMENT |
|
|
|
CHANGE |
|
|
|
|
|
|
|
|
|
|
TERMINATION |
|
|
|
|||||||||||||||||||||
Enrollment/Change Form |
NEW HIRE |
(ATTACH DOCUMENTS) |
CHANGE COVERAGE TYPE |
NAME/ADDRESS CHANGE |
LEFT EMPLOYMENT |
NO LONGER ELIGIBLE |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
LOSS OF INSURANCE |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
ANNUAL OPEN ENROLLMENT |
|
|
|
ADD DEPENDENT LISTED BELOW |
LOSS OF INSURANCE |
VOLUNTARY CANCELLATION |
DECEASED DATE |
||||||||||||||||||||
|
|
PO BOX 9185 • QUINCY, MA 02269 |
COBRA |
|
|
|
TERMINATE DEPENDENT |
|
(ATTACH DOCUMENTS) |
MOVED FROM SERVICE AREA |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
P/T TO F/T DATE |
|
|
|
|
LISTED BELOW |
|
|
|
|
MARRIAGE DATE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
OTHER |
|
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|||||||||||||||||||||
|
|
|
|
|
www.harvardpilgrim.org |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTRACT / ID NUMBER |
|
|
GROUP / COMPANY NAME |
|
|
|
|
|
|
DATE OF HIRE |
|
|
|
|
|
|
DIVISION |
|
|
|
|
|
|
|
EFFECTIVE DATE |
||||||||||
H |
|
P |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
EMPLOYEE NAME |
|
|
|
|
|
|
|
|
|
TYPE OF COVERAGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
FIRST |
MIDDLE |
LAST |
|
|
|
INDIVIDUAL |
|
|
|
MARITAL STATUS |
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
ADDRESS |
|
|
|
|
|
|
|
|
|
FAMILY |
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
APT. NO. |
STREET |
|
PO BOX |
PLEASE USE THE CODES LISTED BELOW TO COMPLETE DEPENDENT RELATION BLOCK |
|
|||
|
|
|
COUNTY |
02 SPOUSE |
03 UNMARRIED CHILD UNDER 19 |
04 |
UNMARRIED STEPCHILD UNDER 19 |
|
|
|
|
|
|
||||
CITY |
|
STATE |
ZIP |
05 * UNMARRIED |
06 |
HANDICAPPED (VERIFICATION REQUIRED) |
07 |
|
TELEPHONE (HOME) |
TELEPHONE (WORK) |
IT IS VERY IMPORTANT THAT EACH MEMBER SELECT A PRIMARY CARE PHYSICIAN. |
||||||
( |
) |
( |
) |
AS A PLAN MEMBER YOU MUST CHOOSE A PRIMARY CARE PHYSICIAN (PCP). IF YOU DO NOT HAVE A PCP, |
||||
|
MOST SPECIALITY CARE MAY NOT BE COVERED. |
|
||||||
|
|
|
|
|
|
|||
|
|
|
DATE OF BIRTH |
|
|
|
|
|
|
|
|
|
|
ARE YOU |
|
|||||
|
LANGUAGE |
|
|
SEX |
RELATION |
SOCIAL SECURITY NUMBER |
SELECT A PRIMARY CARE PHYSICIAN AND |
A REGULAR |
PCP # |
|||||||||||
|
MO |
|
|
DAY |
YR |
|
PATIENT OF |
|||||||||||||
FIRST MI LAST (IF NOT SAME AS EMPLOYEE) |
CODE |
|
|
CODE |
TOWN FOR EACH MEMBER |
|||||||||||||||
|
|
|
|
|
|
|
|
|
THIS DOCTOR? |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
EMPLOYEE |
|
|
|
|
|
|
|
|
M |
F |
O1 |
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPOUSE |
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPENDENT |
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPENDENT |
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPENDENT |
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPENDENT |
|
|
|
|
|
|
|
|
M |
F |
|
|
|
|
|
|
|
Y |
N |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LANGUAGE
CODES
(Optional)
WHAT LANGUAGE DO YOU SPEAK MOST OFTEN? PLEASE LIST THE APPROPRIATE CODE AFTER EACH MEMBER’S NAME. THIS INFORMATION WILL HELP US WORK TOWARD BEST MEETING YOUR NEEDS.
|
AS |
|
CA |
|
|
CV |
|
EN |
|
FR |
|
HA |
|
HM |
|
IT |
|
KH |
|
LO |
|
|
MN |
|
|
PT |
|
|
RU |
|
|
SP |
|
|
VI |
|
OTHER |
|
American |
Sign |
Language |
Cantonese |
|
Cape Verdean |
English |
French |
Haitian |
Hmong |
Italian |
Khmer |
Laotian |
Mandarin |
Portuguese |
Russian |
Spanish |
Vietnamese |
|
Specify |
|||||||||||||||||||
*IF YOU HAVE LISTED A
STUDENT(S) NAME |
NAME OF SCHOOL(S) |
|
|
|
|
|
|
|
|
|
|
THIS INFORMATION MAY BE USED TO VERIFY ELIGIBILITY
HAVE YOU EVER BEEN A MEMBER OF Pilgrim Health Care, Harvard Community Health Plan, HCHP OF NE, HPHC OR HPHC OF NE? YES |
NO |
||
IF YOU WOULD LIKE TO RECEIVE A MENU OF ELECTRONIC WAYS TO INTERACT WITH US, LIST YOUR |
|
||
|
(OPTIONAL) |
|
|
THE
YOUR
I UNDERSTAND THAT MEMBERSHIP WILL BECOME EFFECTIVE UPON ACCEPTANCE BY THE PLAN AND THAT BENEFITS UNDER THE PLAN WILL BE EXPLAINED IN A SEPARATE DOCUMENT. I ALSO UNDERSTAND THAT THE SUBROGATION PROVISION APPLICABLE TO MAINE MEMBERS, OUTLINED IN A SEPARATE DOCUMENT, PERMITS SUBROGATION PAYMENTS ON A JUST AND EQUITABLE BASIS. DURING MY MEMBERSHIP, I AUTHORIZE ANY HEALTH CARE PROVIDER OR OTHER HEALTH PLAN TO PROVIDE MEDICAL INFORMATION AND RECORDS TO THE PLAN, THE PLAN ADMINISTRATOR, OR PLAN AFFILIATED HEALTH CARE PROVIDERS. I ALSO AUTHORIZE THE PLAN, THE PLAN ADMINISTRATION, AND ANY PLAN HEALTH CARE PROVIDERS RENDERING SERVICES TO ME OR MY DEPENDENTS TO RECEIVE COPIES OF MY OR MY DEPENDENTS’ MEDICAL RECORDS. I AUTHORIZE THE USE BY THE PLAN, AND ITS AGENTS, OF ANY INFORMATION OBTAINED HEREUNDER FOR THE DELIVERY OF HEALTH SERVICE, TO DETERMINE ELIGIBILITY AND ENTITLEMENT TO BENEFITS (INCLUDING REIMBURSEMENT BY THIRD PARTIES), FOR EDUCATION AND RESEARCH IN ACCORDANCE WITH GOVERNMENT REGULATIONS, AND FOR THE OTHER PLAN PROFESSIONAL ACTIVITIES SUCH AS UTILIZATION REVIEW, QUALITY ASSURANCE, CASE MANAGEMENT, REFERRAL AND AUTHORIZATION,DISEASE MANAGEMENT, FRAUD DETECTION AND CERTAIN OVERSIGHT ACTIVITIES, SUCH AS ACCREDITATION AND REGULATORY AUDITS. I UNDERSTAND THAT A COPY OF THIS FORM WILL BE GIVEN TO ME, OR TO MY AUTHORIZED REPRESENTATIVE, UPON REQUEST.
NEW HAMPSHIRE BASED GROUPS PLEASE NOTE: THE ENROLLED PARTICIPANT SHALL BE ALLOWED A GRACE PERIOD OF TEN (10) DAYS FOR MAKING ANY PAYMENT DUE UNDER CONTRACT (RSA
It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purpose of defrauding the company. Penalties may include imprisonment, fines or a denial of insurance benefits.
THE EMPLOYEE, SPOUSE AND ALL DEPENDENTS AGE 18 YEARS AND OVER MUST SIGN THIS FORM FOR ENROLLMENT.
EMPLOYEE SIGNATURE |
|
DATE |
|
DEPENDENT SIGNATURE (age 18 years - over) |
|
DATE |
|
DEPENDENT SIGNATURE (age 18 years - over) |
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
SPOUSE SIGNATURE (if applicable) |
|
DATE |
|
DEPENDENT SIGNATURE (age 18 years - over) |
|
DATE |
|
EMPLOYER SIGNATURE |
|
DATE |
10/01 |
WHITE - HARVARD PILGRIM COPY |
YELLOW - EMPLOYER COPY |
PINK - EMPLOYEE COPY |