
de health examen can be filled out without difficulty. Just make use of FormsPal PDF tool to complete the job quickly. To keep our editor on the cutting edge of convenience, we work to put into operation user-oriented features and enhancements on a regular basis. We're at all times thankful for any suggestions - play a vital role in reshaping PDF editing. Should you be looking to get going, here's what you will need to do:
Step 1: First, open the pdf editor by pressing the "Get Form Button" in the top section of this page.
Step 2: With this advanced PDF editing tool, you can actually do more than just complete blank form fields. Try all of the features and make your docs seem perfect with customized text added in, or fine-tune the original content to perfection - all comes along with an ability to add almost any pictures and sign the PDF off.
With regards to the fields of this specific document, here is what you need to do:
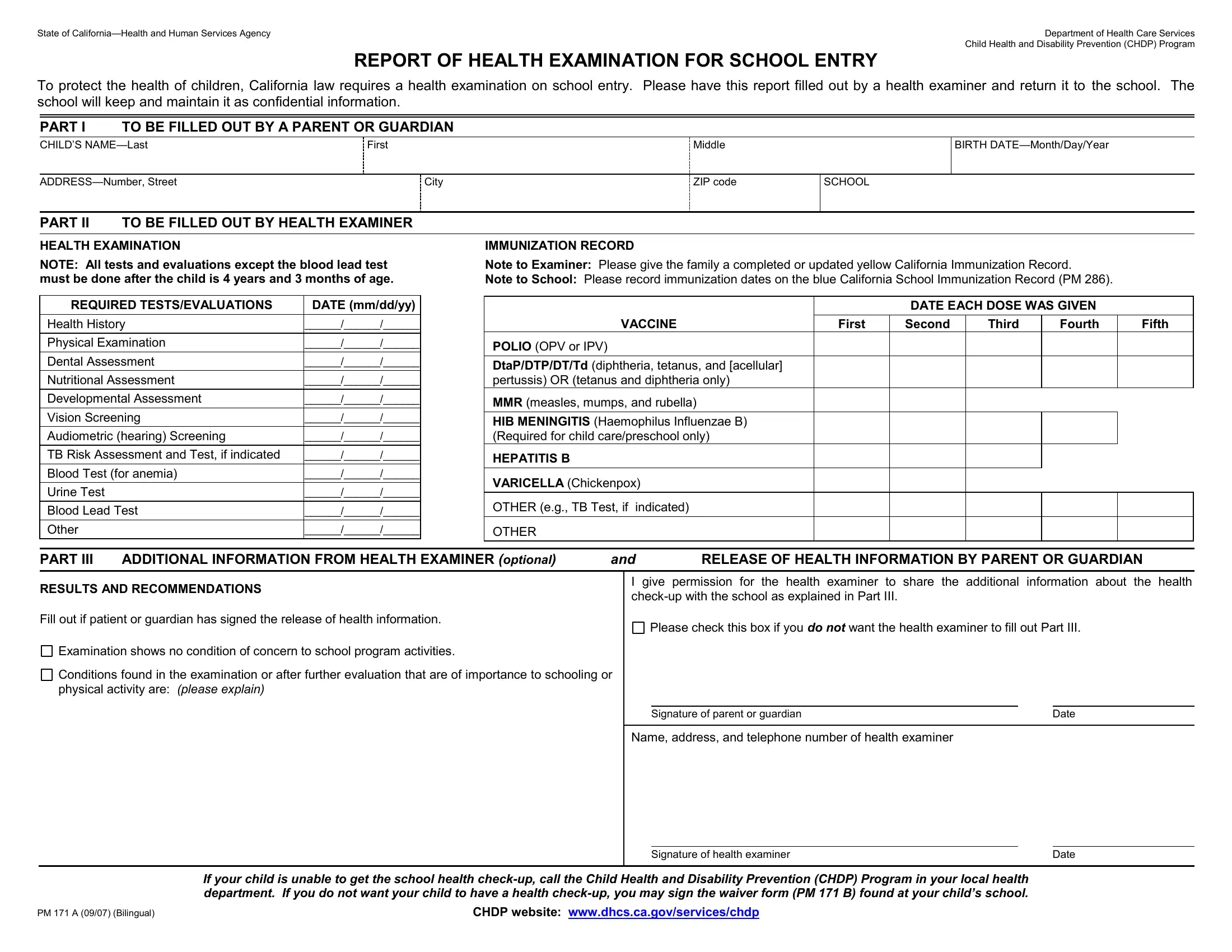
1. First of all, once filling in the de health examen, start out with the part that includes the following blanks:
2. Just after this selection of fields is filled out, go on to enter the applicable information in these: I give permission for the health, Please check this box if you do, RESULTS AND RECOMMENDATIONS Fill, Examination shows no condition of, Conditions found in the, Signature of parent or guardian, Date, Name address and telephone number, Signature of health examiner, Date, PM A Bilingual, CHDP website, and If your child is unable to get the.
Concerning RESULTS AND RECOMMENDATIONS Fill and I give permission for the health, be certain that you get them right here. Both these could be the most important fields in this page.
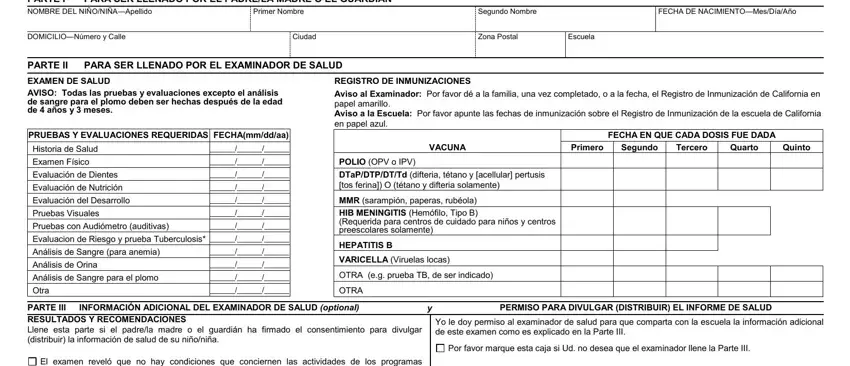
3. This third step is usually straightforward - complete all the blanks in Para proteger la salud de los, PARA SER LLENADO POR EL PADRELA, FECHA DE NACIMIENTOMesDíaAño, Segundo Nombre, Primer Nombre, DOMICILIONúmero y Calle, Ciudad, Zona Postal, Escuela, PARTE II, PARA SER LLENADO POR EL EXAMINADOR, EXAMEN DE SALUD AVISO Todas las, PRUEBAS Y EVALUACIONES REQUERIDAS, REGISTRO DE INMUNIZACIONES Aviso, and VACUNA in order to complete the current step.
4. This fourth part arrives with the following form blanks to fill out: El examen reveló que no hay, Las condiciones encontradas en el, de ser indicado, Firma del padremadre o guardián, Firma del examinador de salud, Fecha, Fecha, Si su niño o niña no puede obtener, en su departamento de salud local, CHDP website, and PM A Bilingual.
Step 3: Check the details you've typed into the blank fields and then click the "Done" button. Find the de health examen once you sign up for a free trial. Conveniently use the pdf file in your personal account page, together with any edits and changes being conveniently preserved! Here at FormsPal, we strive to be sure that all of your information is stored protected.