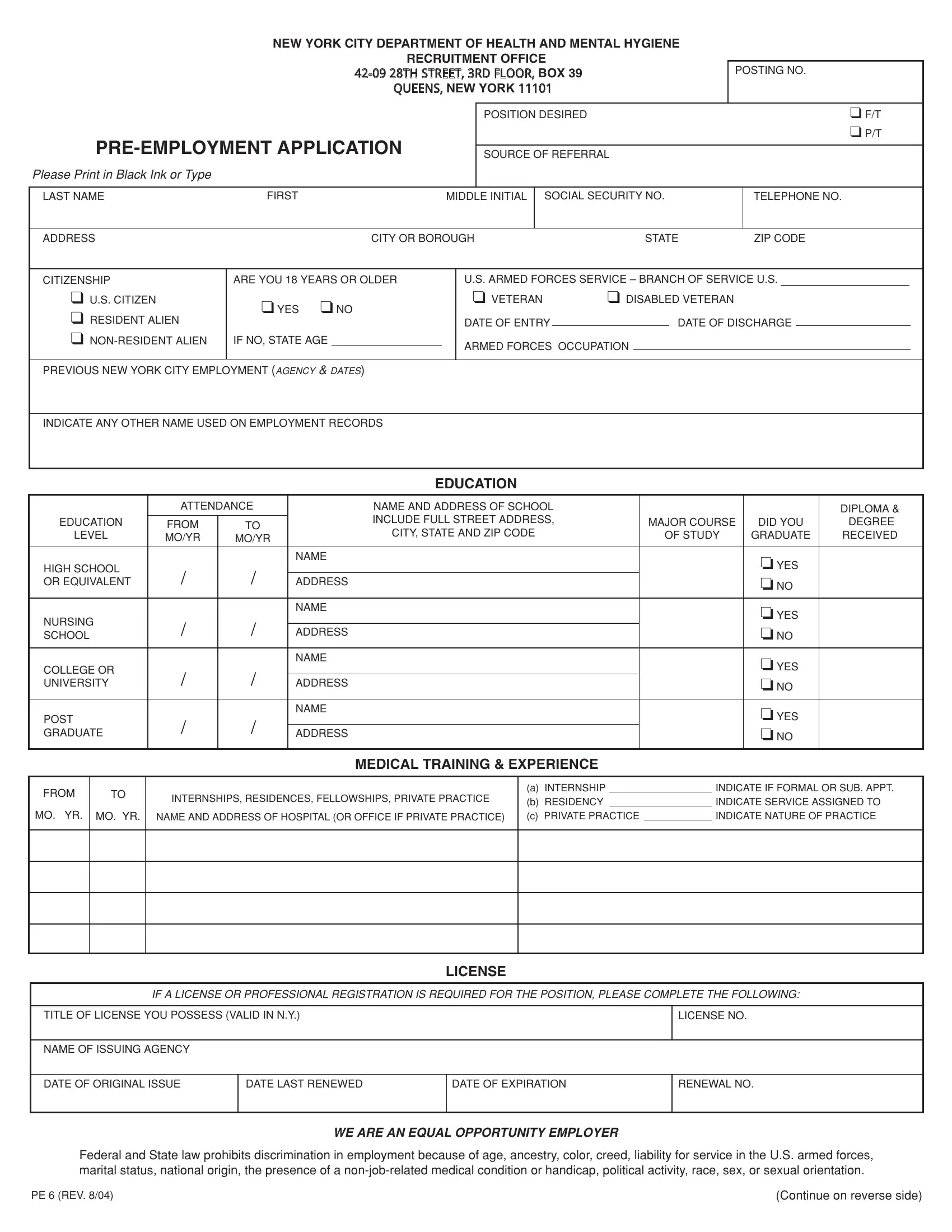
The pre-employment application form serves as an essential medium through which candidates express their interest in job opportunities at the New York City Department of Health and Mental Hygiene. This form, meticulously designed to capture a comprehensive range of information, ensures a systematic approach to the recruitment process. It begins with basic details, including the position desired and the source of referral, and extends to personal information such as citizenship status, age, and military service. Educational backgrounds from high school through postgraduate levels are scrutinized, with a particular emphasis on diplomas, degrees, and fields of study. Moreover, it delves into the medical training and experience of the applicant, highlighting internships, residencies, fellowships, and private practice specifics. Licensure information pertinent to the position sought is requested to confirm qualifications. Employment history is meticulously documented, asking for a detailed account of past roles, responsibilities, supervisory experience, and the reason for leaving past positions. The form additionally inquires about skills, including language proficiencies and clerical capabilities. The declaration at the end of the form underscores the importance of honesty and the implications of providing false information. Adherence to equal opportunity principles is affirmed, indicating a commitment to fairness and legal compliance in hiring. Overall, the pre-employment application form is a crucial document that facilitates an equitable and thorough evaluation of potential employees, ensuring that candidates are assessed based on their qualifications, experiences, and skills relevant to the roles they aspire to fill.
| Question | Answer |
|---|---|
| Form Name | Pre Employment Application Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | new york pre employment form, working papers in new york to print, working papers, printable working papers for minors in ny |
NEW YORK CITY DEPARTMENT OF HEALTH AND MENTAL HYGIENE
RECRUITMENT OFFICE
7+675((75')/225BOX 39 48((16NEW YORK
POSTING NO.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POSITION DESIRED |
|
|
|
|
|
|
|
|
|
|
❑ F/T |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❑ P/T |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
SOURCE OF REFERRAL |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Please Print in Black Ink or Type |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
LAST NAME |
|
|
|
|
|
|
|
|
FIRST |
|
|
|
|
|
MIDDLE INITIAL |
|
|
SOCIAL SECURITY NO. |
|
|
TELEPHONE NO. |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
CITY OR BOROUGH |
|
|
STATE |
|
ZIP CODE |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CITIZENSHIP |
|
|
|
|
|
ARE YOU 18 YEARS OR OLDER |
|
|
|
|
|
U.S. ARMED FORCES SERVICE – BRANCH OF SERVICE U.S. |
|
|
|
|
|
||||||||||||||||||||||||||
|
❑ U.S. CITIZEN |
|
|
|
|
|
|
❑ YES ❑ NO |
|
|
|
|
|
|
❑ VETERAN |
❑ DISABLED VETERAN |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
❑ RESIDENT ALIEN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATE OF ENTRY |
|
|
|
|
DATE OF DISCHARGE |
|
|
|
|
|
|
|
|||||||||||||||
|
❑ |
|
|
|
IF NO, STATE AGE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
ARMED FORCES OCCUPATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
PREVIOUS NEW YORK CITY EMPLOYMENT (AGENCY & DATES) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
INDICATE ANY OTHER NAME USED ON EMPLOYMENT RECORDS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EDUCATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
ATTENDANCE |
|
|
|
|
|
|
NAME AND ADDRESS OF SCHOOL |
|
|
|
|
|
|
|
|
|
|
DIPLOMA & |
|
|||||||||||||||||||
|
EDUCATION |
|
|
FROM |
|
|
|
TO |
|
|
|
|
|
|
INCLUDE FULL STREET ADDRESS, |
|
|
MAJOR COURSE |
|
|
DID YOU |
DEGREE |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
CITY, STATE AND ZIP CODE |
|
|
|
|
|
|||||||||||||||||||||||||||
|
LEVEL |
|
|
MO/YR |
|
|
|
MO/YR |
|
|
|
|
|
OF STUDY |
GRADUATE |
RECEIVED |
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ YES |
|
|
|
|
|
|
|||||
|
HIGH SCHOOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
OR EQUIVALENT |
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ NO |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ YES |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
NURSING |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ NO |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
SCHOOL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ YES |
|
|
|
|
|
|
|||||
|
COLLEGE OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
UNIVERSITY |
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ NO |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ YES |
|
|
|
|
|
|
|||||
|
POST |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
GRADUATE |
|
|
|
|
|
|
|
|
ADDRESS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
❏ NO |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL TRAINING & EXPERIENCE
FROM |
TO |
MO. YR. MO. YR.
INTERNSHIPS, RESIDENCES, FELLOWSHIPS, PRIVATE PRACTICE
NAME AND ADDRESS OF HOSPITAL (OR OFFICE IF PRIVATE PRACTICE)
(a) INTERNSHIP |
|
INDICATE IF FORMAL OR SUB. APPT. |
|
(b) RESIDENCY |
|
INDICATE SERVICE ASSIGNED TO |
|
(c) PRIVATE PRACTICE |
INDICATE NATURE OF PRACTICE |
||
|
|
|
|
LICENSE
IF A LICENSE OR PROFESSIONAL REGISTRATION IS REQUIRED FOR THE POSITION, PLEASE COMPLETE THE FOLLOWING:
TITLE OF LICENSE YOU POSSESS (VALID IN N.Y.)
LICENSE NO.
NAME OF ISSUING AGENCY
DATE OF ORIGINAL ISSUE
DATE LAST RENEWED
DATE OF EXPIRATION
RENEWAL NO.
WE ARE AN EQUAL OPPORTUNITY EMPLOYER
Federal and State law prohibits discrimination in employment because of age, ancestry, color, creed, liability for service in the U.S. armed forces, marital status, national origin, the presence of a
PE 6 (REV. 8/04) |
(Continue on reverse side) |

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYMENT RECORD |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
LIST MOST RECENT EMPLOYMENT FIRST (IF MORE SPACE IS REQUIRED TO ACCOUNT FOR AT LEAST YOUR LAST 10 YEARS OF WORK EXPERIENCE, PLEASE |
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTINUE ON SEPARATE EMPLOYMENT RECORD SHEET AND ATTACH FIRMLY) |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
DATES EMPLOYED |
|
NAME AND ADDRESS OF EMPLOYER |
|
|
|
|
|
|
|
DESCRIPTION OF WORK (INCLUDE NUMBER AND KIND OF EMPLOYEES |
|
|||||||||||||||||
|
|
|
MO. / YR. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPERVISED, IF ANY) |
|
|
|
|||
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TO |
|
PHONE NO. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
|
|
SUPERVISOR'S NAME AND TITLE |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXACT TITLE OF YOUR POSITION |
|
|
|
|
|
ANNUAL SALARY |
|
|
|
|
|
REASON FOR LEAVING |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATES EMPLOYED |
|
NAME AND ADDRESS OF EMPLOYER |
|
|
|
|
|
|
|
DESCRIPTION OF WORK (INCLUDE NUMBER AND KIND OF EMPLOYEES |
|
|||||||||||||||||
|
|
|
MO. / YR. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPERVISED, IF ANY) |
|
|
|
|||
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TO |
|
PHONE NO. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
|
|
SUPERVISOR'S NAME AND TITLE |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXACT TITLE OF YOUR POSITION |
|
|
|
|
|
ANNUAL SALARY |
|
|
|
|
|
REASON FOR LEAVING |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATES EMPLOYED |
|
NAME AND ADDRESS OF EMPLOYER |
|
|
|
|
|
|
|
DESCRIPTION OF WORK (INCLUDE NUMBER AND KIND OF EMPLOYEES |
|
|||||||||||||||||
|
|
|
MO. / YR. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPERVISED, IF ANY) |
|
|
|
|||
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TO |
|
PHONE NO. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
|
|
SUPERVISOR'S NAME AND TITLE |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EXACT TITLE OF YOUR POSITION |
|
|
|
|
|
ANNUAL SALARY |
|
|
|
|
|
REASON FOR LEAVING |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATES EMPLOYED |
|
NAME AND ADDRESS OF EMPLOYER |
|
|
|
|
|
|
|
DESCRIPTION OF WORK (INCLUDE NUMBER AND KIND OF EMPLOYEES |
|
|||||||||||||||||
|
|
|
MO. / YR. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPERVISED, IF ANY) |
|
|
|
|||
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TO |
|
PHONE NO. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
|
|
SUPERVISOR'S NAME AND TITLE |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
EXACT TITLE OF YOUR POSITION |
|
|
|
|
|
ANNUAL SALARY |
|
|
|
|
|
REASON FOR LEAVING |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DATES EMPLOYED |
|
NAME AND ADDRESS OF EMPLOYER |
|
|
|
|
|
|
|
DESCRIPTION OF WORK (INCLUDE NUMBER AND KIND OF EMPLOYEES |
|
|||||||||||||||||
|
|
|
MO. / YR. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUPERVISED, IF ANY) |
|
|
|
|||
|
|
|
FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
TO |
|
PHONE NO. ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
NATURE OF BUSINESS |
|
|
|
|
|
|
|
SUPERVISOR'S NAME AND TITLE |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
EXACT TITLE OF YOUR POSITION |
|
|
|
|
|
ANNUAL SALARY |
|
|
|
|
|
REASON FOR LEAVING |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SKILLS |
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
FOREIGN LANGUAGES |
|
|
|
|
|
|
CLERICAL |
|
|
|
|
|
|
|
ADDITIONAL QUALIFICATIONS |
|
|
|
|
||||||||||
|
|
|
|
|
READ |
WRITE |
SPEAK |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
❏ |
❏ |
❏ |
|
|
TYPING |
|
|
|
|
WPM |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
❏ |
❏ |
❏ |
|
|
SHORTHAND |
|
|
|
WPM |
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
❏ |
❏ |
❏ |
|
|
TRANSCRIPTION |
|
WPM |
|
|
|
|
|
MINIMUM SALARY REQUIREMENTS |
|
PER ❏ HOUR |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
❏ YEAR |
|||||||||||||||||||
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICANT’S CERTIFICATION AND AGREEMENT – PLEASE READ CAREFULLY, SIGN AND DATE BELOW
I certify that the information I have provided in this employment application is correct and complete to the best of my knowledge. I realize that my willful omission or any misrepresentation of facts will be just cause for the rejection of this application or the termination of my services after employment. I understand that any employment which may be offered to me will be on a probationary basis and will be contingent upon my passing a physical examination and verification of my education records and employment history. I agree to cooperate and release those supplying any information from all liability.
|
|
|
APPLICANT’S FULL SIGNATURE |
|
|
DATE SIGNED |
|
|
|
|
Thank you for completing this application. |
|
|
|
|||||
|
It will be kept on file for one year ONLY! |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MAIL TO: |
NYC DEPARTMENT OF HEALTH AND MENTAL HYGIENE |
|
7+675((7 5')/225 BOX 39 |
PE 6 (REV. 8/04) |
QUEENS, NEW YORK 11101 |