
You can use our PDF editor to fill in the dog vaccination form quickly, or download it and fill it out later.
Here are the steps to fill out this template:
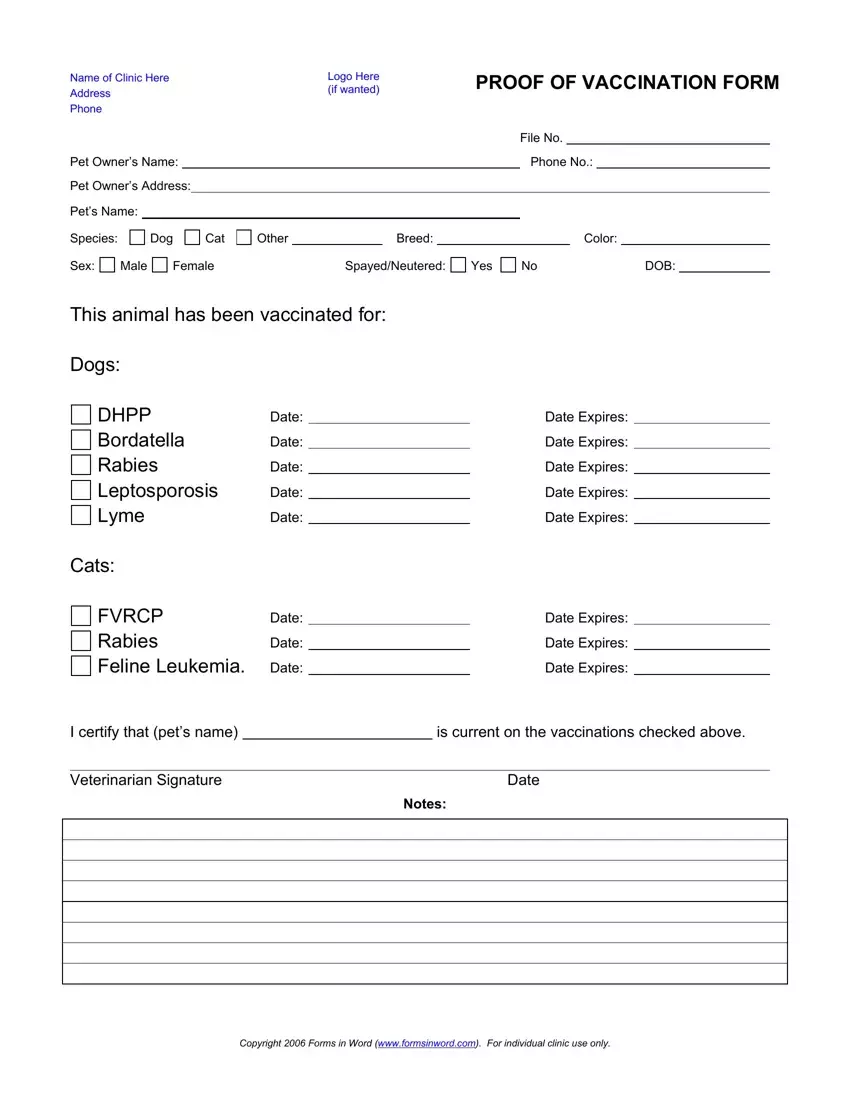
1. Veterinary Clinic
First off, fill in the vet clinic's name, address, and phone number at the top of the form. If they've got a logo or a special clinic code (vaccination form file No.), add either of those on too.
2. Pet Owner
Next up, fill in the pet owner's name, phone number, and address. This bit is very important as it shows who the pet belongs to and is often required by landlords, boarding places, etc.
3. Animal Details
Put in the animal's name and choose the correct species (Dog, Cat, or Other). Then fill in the rest of the details - breed, colour, sex, if they've been spayed/neutered, and when they were born.
4. Shot Records
In the vaccination bit, write down each vaccine your pet has had, including:
• When the vet gave the vaccine
• When it runs out
Common entries include DHPP, Bordetella, Rabies vaccination, Leptospirosis, and Lyme - make sure all the dates are right and legible
For cats, you fill in the feline vaccination fields, and for other animals, fill in the required vaccines as per local regulations or the vet's advice.
5. Certification and Veterinarian's Signature
A licensed vet has to sign and date the certification bit to say the vaccination record is true.
6. Additional Notes
Vets often use this area to explain a pet's vaccination status or anything else that might be relevant.
Some things they might include are:
• Medical reasons for not giving a certain vaccine - with an explanation of course
• Any reaction to the vaccine, or any sensitivities you've noticed
• Booster schedules or follow-on vaccination advice
• Health conditions or age that might affect how your pet is vaccinated
• Titer test results or alternative vaccination plans
• Any other reasons why your pet might need special treatment, such as a travel requirement, an incomplete vaccination series, or instructions for follow-up appointments.
