

Handling PDF documents online is certainly a piece of cake with our PDF tool. You can fill out cims here effortlessly. To make our tool better and more convenient to utilize, we consistently develop new features, taking into account suggestions coming from our users. It just takes a couple of simple steps:
Step 1: Hit the orange "Get Form" button above. It is going to open our pdf tool so you could start filling in your form.
Step 2: With our handy PDF tool, it is easy to accomplish more than simply complete blank fields. Express yourself and make your documents appear professional with custom text put in, or adjust the original input to perfection - all that supported by an ability to incorporate your personal photos and sign the PDF off.
It is actually an easy task to fill out the document with this helpful tutorial! Here is what you should do:
1. Whenever filling out the cims, make certain to complete all essential blanks in their relevant form section. It will help facilitate the process, enabling your details to be processed without delay and accurately.
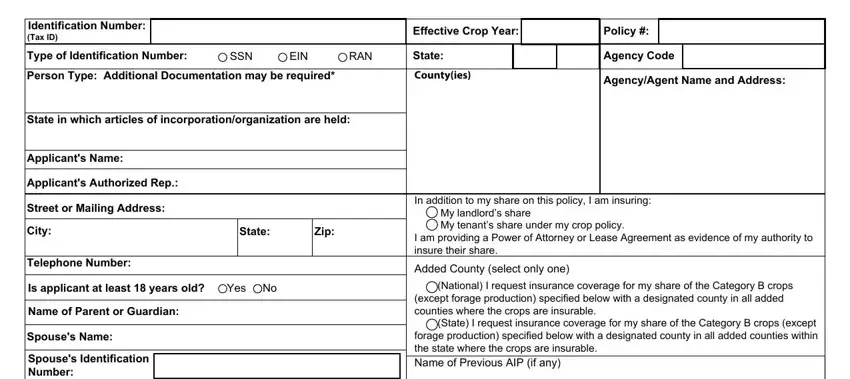
2. The next step is usually to fill out these particular blank fields: Applicants Additional Telephone, Previous Policy Number under, Applicants Email Address, List all persons with a, Name, ID Number Type, LandlordTenant, Person Type, Address, Telephone, Yes, Yes, Yes, Please Complete a SOCIAL SECURITY, and NEW PRODUCER.
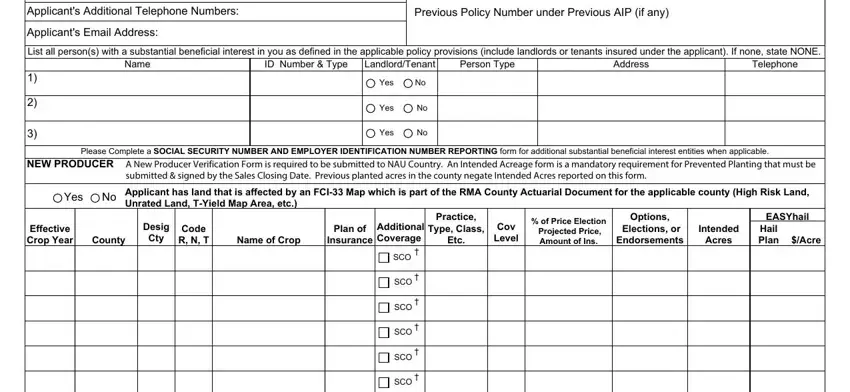
It is possible to get it wrong while filling out your LandlordTenant, and so make sure you take a second look before you finalize the form.
3. Completing Authority to sign crop insurance, Name, Address, Telephone, Grant, Remove, This policy shall continue for, If selecting SCO please complete, APSCM, documentsnaucountrycom Fax to, and Page of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

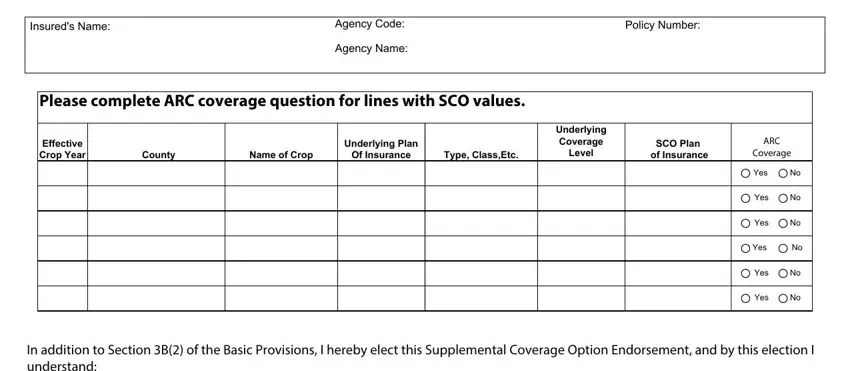
4. The next subsection arrives with the following form blanks to fill out: Insureds Name, Agency Code Agency Name, Policy Number, Please complete ARC coverage, Effective Crop Year, County, Name of Crop, Of Insurance, Type ClassEtc, Underlying Plan, Underlying Coverage, Level, SCO Plan, of Insurance, and ARC.
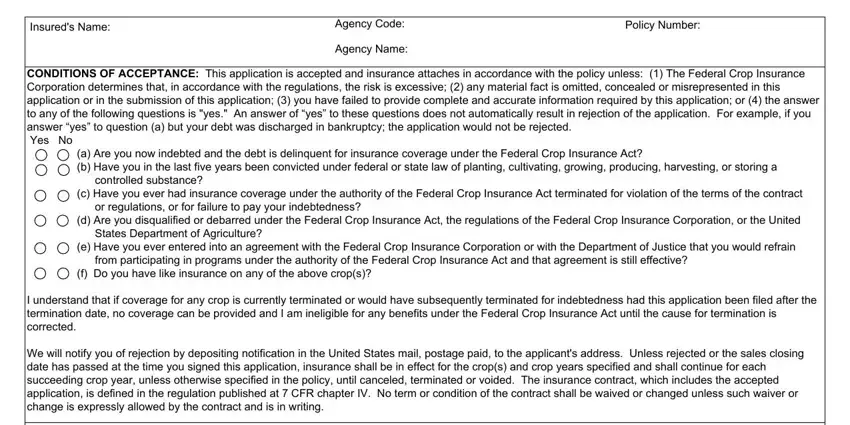
5. As you draw near to the conclusion of the document, there are a couple more requirements that must be satisfied. Particularly, Insureds Name, Agency Code Agency Name, Policy Number, d Are you disqualified or debarred, c Have you ever had insurance, a Are you now indebted and the, CONDITIONS OF ACCEPTANCE This, e Have you ever entered into an, and f Do you have like insurance on should all be done.
Step 3: Make sure that your information is accurate and click on "Done" to progress further. Grab the cims as soon as you sign up for a 7-day free trial. Conveniently access the pdf document inside your personal cabinet, with any modifications and changes automatically preserved! FormsPal ensures your data confidentiality via a protected method that never saves or shares any type of personal data used in the PDF. Rest assured knowing your docs are kept confidential each time you work with our editor!