The QME 104 form serves as a crucial document within California's workers' compensation system, detailing the necessary steps for the reappointment of a Qualified Medical Evaluator (QME). This form is meticulously designed to capture a comprehensive range of information, starting from basic identification and contact details to specific professional qualifications and licenses. It is crafted to ensure that the applicant meets specific criteria set by the Administrative Director of the Division of Workers' Compensation - Medical Unit, ensuring a high standard of medical evaluation for workers' compensation cases. For physicians, particularly M.D.s and D.O.s, the form delves into their board certifications, postgraduate training, and their standing as of June 30, 2000, requiring detailed documentation for verification. Furthermore, it explores the applicant's professional engagements, asking them to affirm their dedication to medical practice, possibly beyond their role as a QME. This includes stipulations about dedicating a significant portion of their practice to direct medical treatment, previous involvements as an Agreed Medical Evaluator, or their affiliations with academic institutions. Additionally, the form mandates disclosures regarding any potential conflicts of interest, financial interests in referred facilities, and convictions that might impact their practice. By initialing affirmative statements regarding these aspects, applicants attest to their compliance with ethical and professional standards. Lastly, the QME 104 form necessitates the listing of recent continuing education courses and insists on the thorough accuracy of the provided information, signifying the importance of ongoing professional development and integrity in the reappointment process.
| Question | Answer |
|---|---|
| Form Name | Qme Form 104 |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | crpf medical claim form 103, ssb medical form 104, 104 pdf, crpf medical claim form 104 |
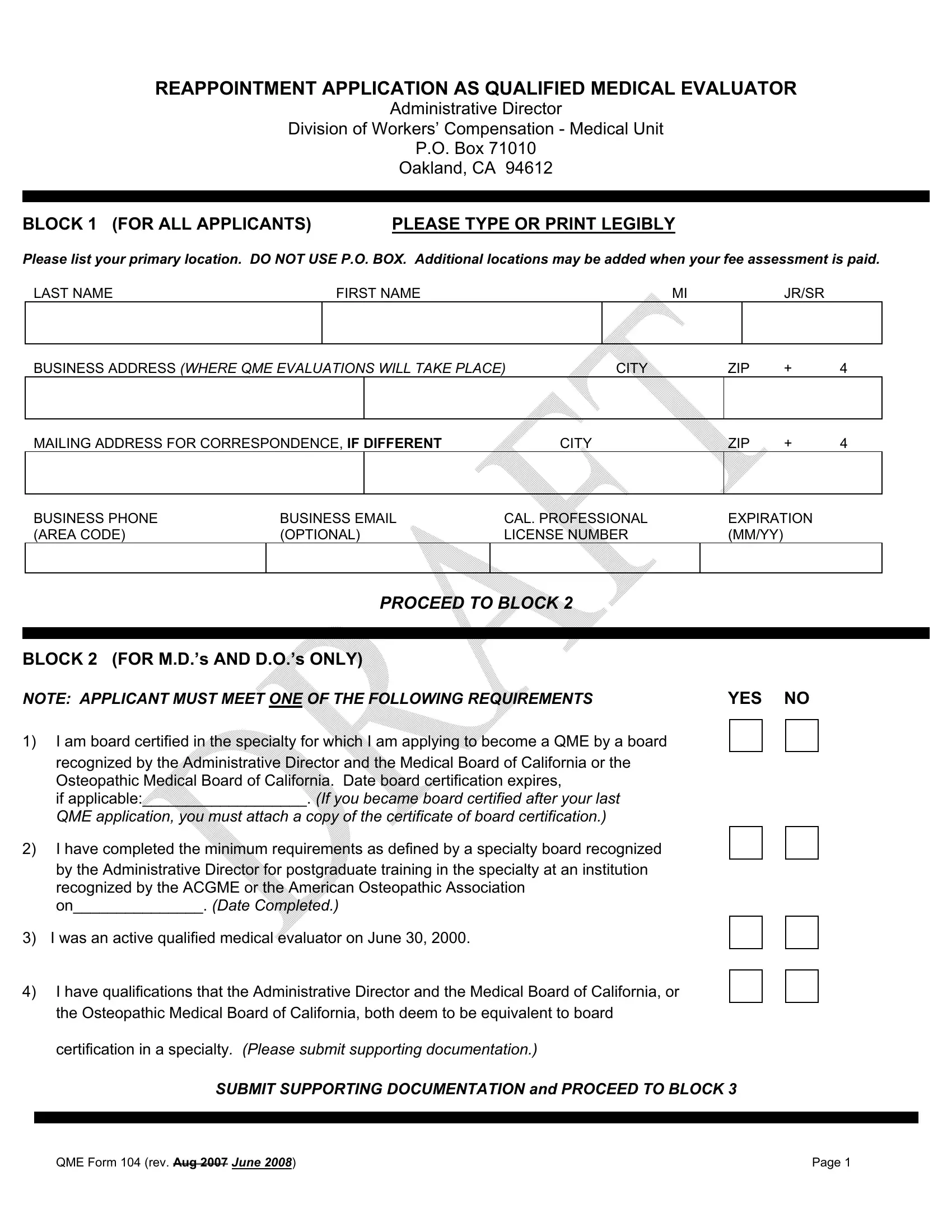
REAPPOINTMENT APPLICATION AS QUALIFIED MEDICAL EVALUATOR
Administrative Director
Division of Workers’ Compensation - Medical Unit
P.O. Box 71010
Oakland, CA 94612
BLOCK 1 (FOR ALL APPLICANTS) |
PLEASE TYPE OR PRINT LEGIBLY |
Please list your primary location. DO NOT USE P.O. BOX. Additional locations may be added when your fee assessment is paid.
LAST NAME |
FIRST NAME |
MI |
JR/SR |
|
|
|
|
BUSINESS ADDRESS (WHERE QME EVALUATIONS WILL TAKE PLACE) |
CITY |
ZIP |
+ |
4 |
||||
|
|
|
|
|
|
|
|
|
MAILING ADDRESS FOR CORRESPONDENCE, IF DIFFERENT |
|
CITY |
ZIP |
+ |
4 |
|||
|
|
|
|
|
|
|
||
BUSINESS PHONE |
BUSINESS EMAIL |
CAL. PROFESSIONAL |
EXPIRATION |
|
||||
(AREA CODE) |
(OPTIONAL) |
LICENSE NUMBER |
(MM/YY) |
|
|
|||
|
|
|
|
|
|
|
|
|
PROCEED TO BLOCK 2
BLOCK 2 (FOR M.D.’s AND D.O.’s ONLY)
NOTE: APPLICANT MUST MEET ONE OF THE FOLLOWING REQUIREMENTS |
YES NO |
|||
1) |
I am board certified in the specialty for which I am applying to become a QME by a board |
|
|
|
|
|
|
||
|
recognized by the Administrative Director and the Medical Board of California or the |
|
|
|
|
Osteopathic Medical Board of California. Date board certification expires, |
|
|
|
|
if applicable:___________________. (If you became board certified after your last |
|
|
|
|
QME application, you must attach a copy of the certificate of board certification.) |
|
|
|
2) |
I have completed the minimum requirements as defined by a specialty board recognized |
|
|
|
|
by the Administrative Director for postgraduate training in the specialty at an institution |
|
|
|
|
recognized by the ACGME or the American Osteopathic Association |
|
|
|
|
on_______________. (Date Completed.) |
|
|
|
3) |
I was an active qualified medical evaluator on June 30, 2000. |
|
|
|
4) |
I have qualifications that the Administrative Director and the Medical Board of California, or |
|
|
|
|
|
|
||
|
the Osteopathic Medical Board of California, both deem to be equivalent to board |
|
|
|
certification in a specialty. (Please submit supporting documentation.)
SUBMIT SUPPORTING DOCUMENTATION and PROCEED TO BLOCK 3
QME Form 104 (rev. Aug 2007 June 2008) |
Page 1 |
BLOCK 3 (FOR ALL APPLICANTS)
NOTE: APPLICANT MUST MEET ONE OF THE FOLLOWING REQUIREMENTS |
Check One |
1)I devote at least
(“Direct Medical Treatment” is that special phase of the
effects of an industrial injury.)
2)I have served as an Agreed Medical Evaluator (AME) on eight (8) or more occasions in the 12 months prior to submitting this application. (Submit documentation of 8 AMEs, i.e. AME cover letters, first page of reports or a sworn statement made under penalty of perjury.)
3)I am currently a salaried faculty member at an accredited university or college. I have a current California license to practice as a physician and have been engaged in teaching, lecturing, published writing or medical research at that university or college in my area of specialty
for not less than
4)I am retired from active practice. I have a minimum of 25 years’ experience in practice as a physician and, currently, I practice fewer than 10 hours per week on direct medical treatment as a physician. My practice in the three consecutive years immediately preceding the time of reappointment was not devoted solely to the forensic evaluation of disability.
5)I am retired from active practice due to a documented medical or physical disability as defined by Government Code §12926 and currently practicing in my specialty fewer than 10 hours per week. I have 10 years’ experience in workers’ compensation medical issues as a physician. My practice in the three consecutive years immediately preceding the time of application was not devoted solely to the forensic evaluation of disability. (Please submit medical documentation of your disability.)
SUBMIT SUPPORTING DOCUMENTATION and PROCEED TO BLOCK 4
BLOCK 4 (FOR ALL APPLICANTS)
PLEASE INDICATE SPECIALTY(IES) FOR WHICH YOU ARE APPLYING TO DO QME EXAMS. (PLEASE USE SPECIALTY CODE LIST ATTACHED TO THIS FORM.)
Professional practice |
Professional practice |
Professional practice |
|
specialty code |
specialty code |
specialty code |
|
|
|
|
|
PROCEED TO BLOCK 5
QME Form 104 (rev. Aug 2007 June 2008) |
Page 2 |
BLOCK 5 (FOR ALL APPLICANTS)
Affirmations: (Initialing each box affirms that you have read and agree to each of the statements. Do not initial if your statement is untrue; attach explanation on a separate piece of paper. I understand that in such cases I may be subject to Failure to do so may result in disciplinary action by the Administrative Director.)
INITIAL
EACH BOX
A.License Status and Convictions (Present and past)
My California license to practice medicine as a physician is active and is neither restricted nor encumbered by suspension, interim suspension or probation. I certify that I have not been convicted of either a misdemeanor or felony related to my practice or for a crime of moral turpitude.
B.License Status and Convictions (Future changes)
I agree to notify the Administrative Director if my California license to practice medicine is placed on suspension, interim suspension, probation or is restricted by my licensing agency. I further agree to notify the Administrative Director if I am convicted of a misdemeanor or felony related to my practice or a crime of moral turpitude. I understand that the Administrative Director may take disciplinary action or may deny my application for reappointment if my license is on probation with my licensing authority.
C.Referrals, Specified Financial Interests, Other Prohibited Activities
I agree that I shall abide by all Administrative Director regulations. I have read and understand Labor Code Sections 139.3 and 139.31. I agree that I shall abide by all their provisions. I will not refer patients to facilities in which I or my family members have a financial interest, except as permitted by law. I agree I shall not offer, deliver, receive or accept any rebate, refund, commission, preference, patronage, dividend, discount or other consideration, whether in the form of money or otherwise, as compensation or inducement for any referred evaluation or consultation. I agree not to solicit to provide medical treatment to an injured employee for any injury for which I have done a QME evaluation. I have not performed a QME evaluation while not certified by the Administrative Director as a QME. I have accurately and fully reported all specified financial interests that may affect the fairness of QME panels, as required on the attached QME SFI Form 124. I declare I spend five or more hours per week in direct medical treatment (or, for QMEs appointed under the AME, retired or faculty status, in other specified activity) at each location I have listed as a “primary practice” location.
D.Continuing Education Courses
List the continuing education courses you have completed within the last 24 months:
Name of Provider |
|
Name of Course |
|
Date(s) |
|
Number of Credits |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Verification
I have used all reasonable diligence in preparing and completing this application. I have reviewed this completed application and to the best of my knowledge the information contained herein and in the attached supporting documentation is true, correct and complete. I declare under penalty of perjury under the laws of the State of California that the foregoing is true and correct. (Failure to provide truthful information shall result in denial of applicant’s reappointment and/or disciplinary action.)
Executed on |
at |
, |
CA |
||||
|
|
|
|
|
|
|
|
|
(MM/DD/YY) |
|
County |
|
|
|
Applicant’s Signature |
QME Form 104 (rev. Aug 2007 June 2008) |
|
|
|
|
|
Page 3 |
|

A PUBLIC DOCUMENT
PRIVACY NOTICE - The Information Practices Act of 1977 and the Federal Privacy Act require the Administrative Director to provide the following notice to individuals who are asked by a governmental entity to supply information for appointment as a Qualified Medical Evaluator (QME).
The principal purpose for requesting information from QMEs is to administer the QME program within the California workers' compensation system. Additional information may be requested if your application is denied and/or a disciplinary action is taken.
The California Labor Code requires every QME physician to meet certain statutory requirements. Physicians are required by the Labor Code to provide: name; business address/addresses; professional education; training; license number; year entered practice and other requirements deemed necessary by the Administrative Director. It is mandatory to furnish all the appropriate information requested by the Administrative Director. Failure to provide all of the requested information may result in the denial of the application.
As authorized by law, information furnished on this form may be given to: you, upon request; the public, pursuant to the Public Records Act; a governmental entity, when required by state or federal law; to any person, pursuant to a subpoena or court order or pursuant to any other exception in Civil Code § 1798.24.
An individual has a right of access to records containing his/her personal information that are maintained by the Administrative Director. An individual may also amend, correct, or dispute information in such personal records (Civil Code §
Requests should be sent to:
Division of Workers'
P.O. Box 71010
Oakland, CA 94612
(510)
Fax: (510)
You may request a copy of the Division of Workers' Compensation policy and procedures for inspection of records at the above address. Copies of the procedures and all records are ten cents ($0.10) per page, payable in advance. (Civil Code § 1798.33).
QME Form 104 (rev. Aug 2007 June 2008) |
Page 4 |

For Use on the QME Reappointment Application Form 104
IMPORTANT: PLEASE USE THREE LETTER SPECIALTY CODE WHEN
COMPLETING BLOCK 4 OF THE REAPPOINTMENT APPLICATION FORM
|
MD/DO SPECIALTY CODES |
|
|
MAI |
Allergy & Immunology |
MTO |
Otolaryngology |
MPA |
Anesthesiology - Pain Medicine |
MPA |
Pain Medicine |
MDE |
Dermatology |
MHA |
Pathology |
MAI |
Dermatology - Allergy & Immunology |
MEP |
Pediatrics |
MEM |
Emergency Medicine |
MAI |
Pediatrics - Allergy & Immunology |
MTT |
Emergency Medicine - Toxicology |
MPR |
Physical Medicine & Rehabilitation |
MFP |
Family Practice |
MPA |
Physical Medicine & Rehabilitation – |
|
|
|
Pain Medicine |
MPM |
General Preventive Medicine |
MPS |
Plastic Surgery (other than Hand) |
MPT |
General Preventive Medicine – Toxicology |
MHH |
Plastic Surgery - Hand |
MTT |
|
|
|
MMM |
Internal Medicine |
MPD |
Psychiatry (other than Pain Medicine) |
MAI |
Internal Medicine - Allergy & Immunology |
MPA |
Psychiatry – Pain Medicine |
MMV |
Internal Medicine - Cardiovascular Disease |
MMO |
Radiology - Oncology |
MME |
Internal Medicine – Endocrinology |
MSY |
Surgery (other than Spine or Hand) |
|
Diabetes & Metabolism |
|
|
MMG |
Internal Medicine - Gastroenterology |
MHH |
Surgery - Hand |
MMH |
Internal Medicine - Hematology |
MSG |
Surgery - General Vascular |
MMI |
Internal Medicine - Infectious Disease |
MTS |
Thoracic Surgery |
MMO |
Internal Medicine - Medical Oncology |
MUU |
Urology |
MMN |
Internal Medicine - Nephrology |
|
|
MMP |
Internal Medicine - Pulmonary Disease |
|
|
MMR |
Internal Medicine - Rheumatology |
|
|
MPN |
Neurology |
ACA |
Acupuncture |
MPA |
Neurology - Pain Medicine |
DCH |
Chiropractic |
MNS |
Neurological Surgery (other than Spine) |
DEN |
Dentistry |
MNB |
Neurological Surgery – Spine |
OPT |
Optometry |
MOG |
Obstetrics & Gynecology |
POD |
Podiatry |
MPO |
Occupational Medicine |
PSY |
Psychology |
MTT |
Occupational Medicine – Toxicology |
PSN |
Psychology - Clinical Neuropsychology |
MOP |
Ophthalmology |
|
|
MOS |
Orthopaedic Surgery (other than Spine or |
|
|
|
Hand) |
|
|
MNB |
Orthopaedic Surgery - Spine |
|
|
MHH |
Orthopaedic Surgery – Hand |
|
|
MMO |
Orthopaedic Surgery - Oncology |
|
|
QME Form 104 (rev. Aug 2007 June 2008) |
Page 5 |