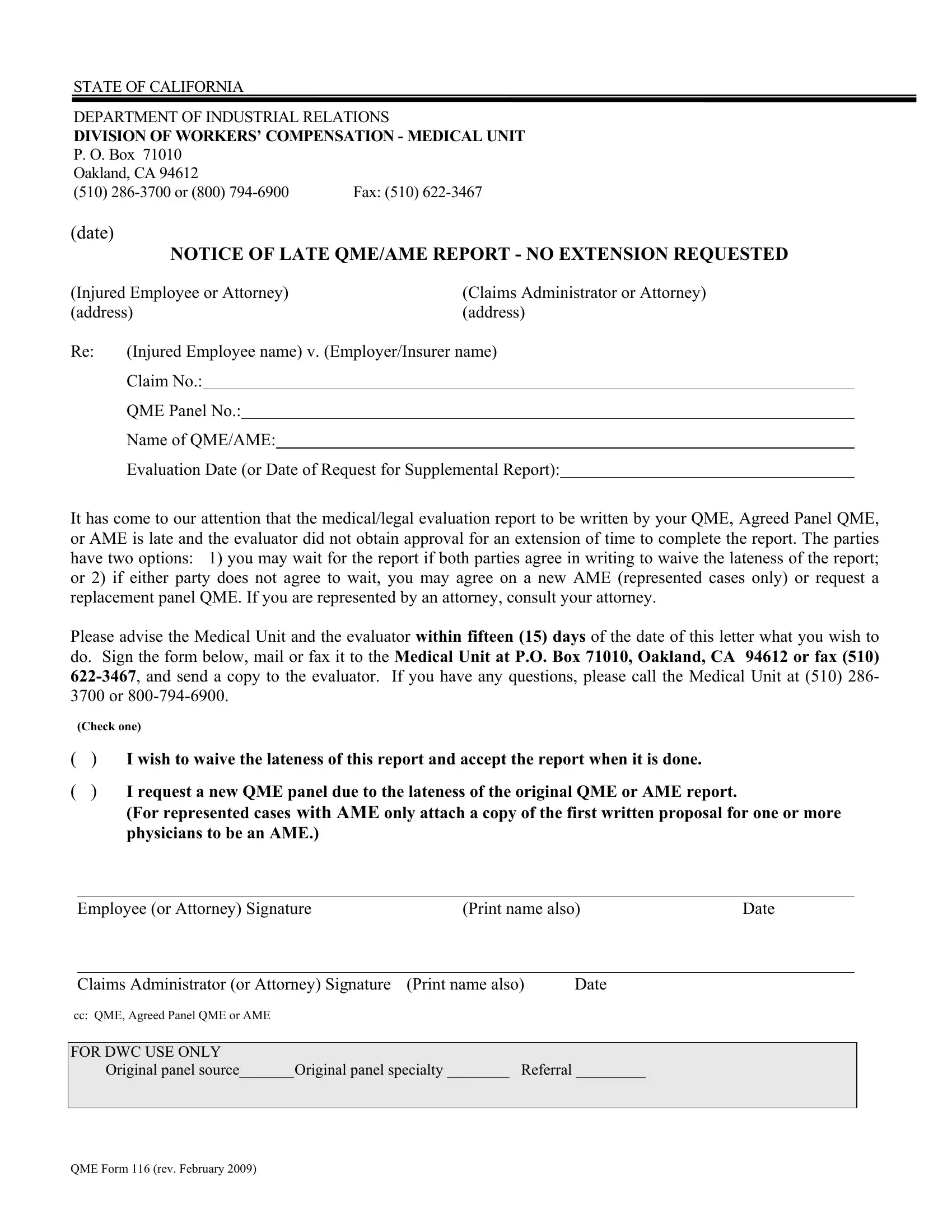
At the heart of California's Workers' Compensation system, the processing of claims and ensuring timely contributions from medical evaluators is critical. The QME 116 form, issued by the State of California Department of Industrial Relations Division of Workers' Compensation Medical Unit, serves as a pivotal document in this process. It addresses situations where medical or legal evaluation reports by a Qualified Medical Evaluator (QME), Agreed Medical Evaluator (AME), or an Agreed Panel QME are delayed without an approved extension request. Originating from Oakland, California, this form notifies both the injured employee (or their attorney) and the claims administrator (or their attorney) of the delay, outlining specific actions that can ensue. These include the options to either mutually waive the report's tardiness or to proceed by requesting a new AME or a replacement panel QME. The form further emphasizes the need for clear communication and timely decision-making, providing a 15-day window for the involved parties to respond to the notice. Additionally, it includes sections for signatures from both the employee or their representative and the claims administrator or their representative, ensuring that all decisions are officially documented. The form not only facilitates the smooth operation of workers’ compensation evaluations but also underscores the importance of accountability and efficiency in handling injured workers' claims.
| Question | Answer |
|---|---|
| Form Name | Qme Form 116 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form 116, evaluator, physicians, Referral |
STATE OF CALIFORNIA
DEPARTMENT OF INDUSTRIAL RELATIONS
DIVISION OF WORKERS’ COMPENSATION - MEDICAL UNIT
P. O. Box 71010 |
|
Oakland, CA 94612 |
|
(510) |
Fax: (510) |
(date)
NOTICE OF LATE QME/AME REPORT - NO EXTENSION REQUESTED
(Injured Employee or Attorney) |
(Claims Administrator or Attorney) |
||
(address) |
(address) |
||
Re: |
(Injured Employee name) v. (Employer/Insurer name) |
||
|
Claim No.: |
|
|
QME Panel No.:
Name of QME/AME:
Evaluation Date (or Date of Request for Supplemental Report):
It has come to our attention that the medical/legal evaluation report to be written by your QME, Agreed Panel QME, or AME is late and the evaluator did not obtain approval for an extension of time to complete the report. The parties have two options: 1) you may wait for the report if both parties agree in writing to waive the lateness of the report; or 2) if either party does not agree to wait, you may agree on a new AME (represented cases only) or request a replacement panel QME. If you are represented by an attorney, consult your attorney.
Please advise the Medical Unit and the evaluator within fifteen (15) days of the date of this letter what you wish to do. Sign the form below, mail or fax it to the Medical Unit at P.O. Box 71010, Oakland, CA 94612 or fax (510)
(Check one)
() I wish to waive the lateness of this report and accept the report when it is done.
() I request a new QME panel due to the lateness of the original QME or AME report.
(For represented cases with AME only attach a copy of the first written proposal for one or more physicians to be an AME.)
Employee (or Attorney) Signature |
(Print name also) |
Date |
Claims Administrator (or Attorney) Signature (Print name also) |
Date |
cc: QME, Agreed Panel QME or AME |
|
FOR DWC USE ONLY
Original panel source_______Original panel specialty ________ Referral _________
QME Form 116 (rev. February 2009)