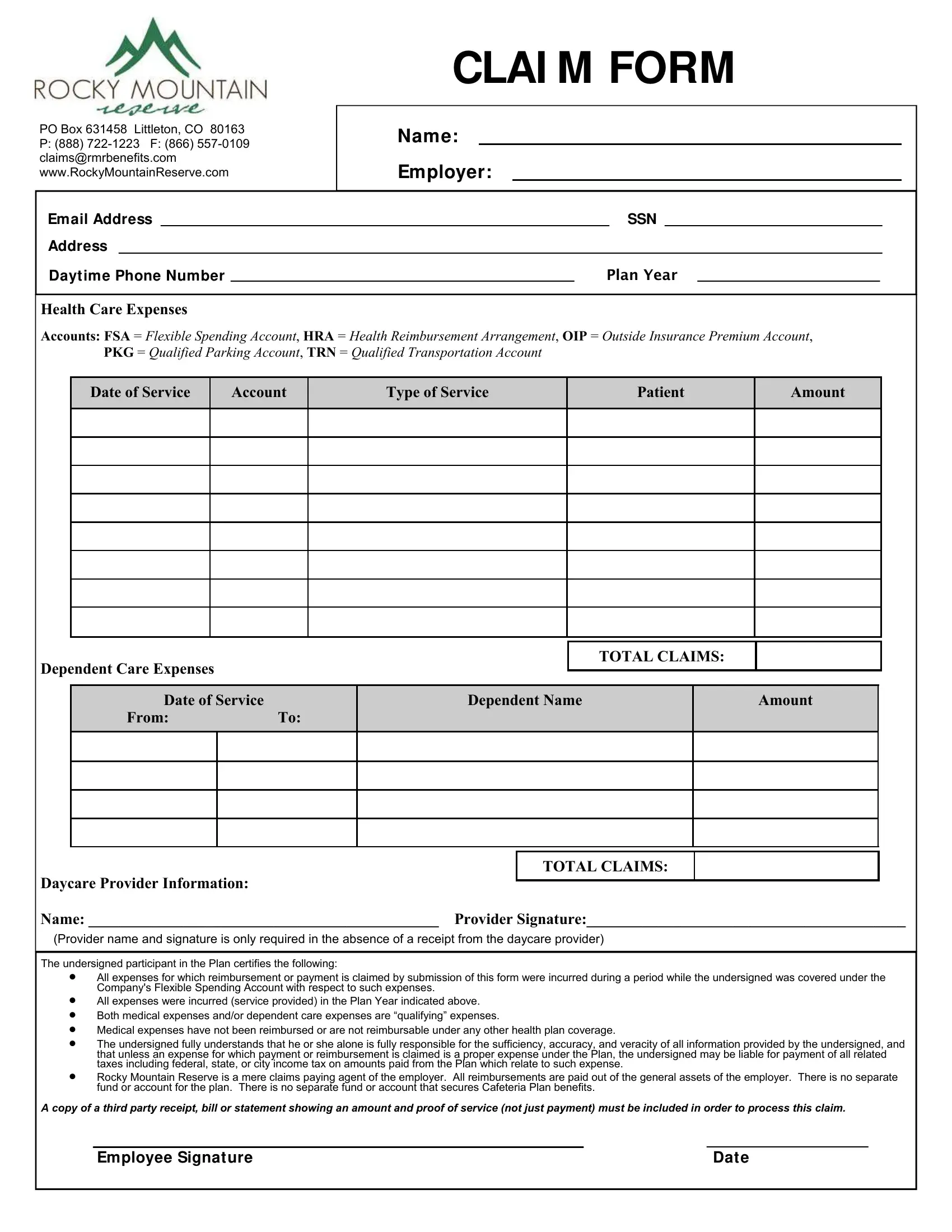
Navigating through the complexities of healthcare and dependent care expenses can often feel like an uphill battle. With the introduction of forms like the Rocky Mountain Claim form, strides have been made towards simplifying the reimbursement process for these critical expenses. This form serves as a key tool for individuals covered under a company's Flexible Spending Account (FSA), allowing them to claim reimbursement for qualifying healthcare and dependent care expenses incurred within a specified Plan Year. It underscores the importance of submitting accurate and truthful information, as the person filling out the form bears sole responsibility for the data provided. Highlighting a stringent verification process, it requires the inclusion of third-party receipts or statements as proof of service to ensure that only legitimate claims are reimbursed. Rocky Mountain Reserve, acting as the claims paying agent, facilitates the reimbursement process directly from the general assets of the employer, emphasizing that there is no separate fund or account designated for the plan benefits. This form encapsulates a crucial aspect of managing healthcare and dependent care expenditures, thereby providing a structured pathway for individuals to navigate their claims within the framework of an FSA, thereby underscoring its importance in the broader context of personal financial planning and healthcare management.
| Question | Answer |
|---|---|
| Form Name | Rocky Mountain Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | rockymountainreserve com, rocky mountain reserve fsa login, rocky mountain spotted fever forms for disability to be off work, forms |
CLAI M FORM
PO Box 631458 Littleton, CO 80163
P:(888)
Name:
Employer:
|
Email Address |
|
|
|
SSN |
|
|
|
||
|
Address |
|
|
|
|
|
|
|
|
|
|
Dayt ime Phone Number |
|
PLAN YEAR |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Health Care Expenses
Accounts: FSA = Flexible Spending Account, HRA = Health Reimbursement Arrangement, OIP = Outside Insurance Premium Account, PKG = Qualified Parking Account, TRN = Qualified Transportation Account
Date of Service
Account
Type of Service
Patient
Amount
Dependent Care Expenses |
|
|
|
TOTAL CLAIMS: |
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
Date of Service |
|
Dependent Name |
|
|
Amount |
|
||
|
From: |
To: |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Daycare Provider Information:
TOTAL CLAIMS:
Name: _____________________________________________ Provider Signature:_________________________________________
(Provider name and signature is only required in the absence of a receipt from the daycare provider)
The undersigned participant in the Plan certifies the following:
A copy of a third party receipt, bill or statement showing an amount and proof of service (not just payment) must be included in order to process this claim.
Employee Signature |
Date |