In the heart of ensuring a healthy and secure environment for both students and volunteers within its educational establishments, the San Diego Unified School District mandates a comprehensive tuberculosis screening process for all its volunteers. This rigorous procedure is encapsulated in the San Diego Tb Test Form, a key document that volunteers must accurately fill out and submit. The form requires detailed information, including the volunteer's name, date of birth, usual volunteer location, home address, and contact details, ensuring a clear identification and traceability of each volunteer's health status. With an intradermal tuberculin test at its core, the form serves not only as a record of the test administered but also highlights the importance of a 48-72 hour reading post-administration. A crucial aspect of this form is the certification of tuberculosis examination by a licensed physician and surgeon, confirming the volunteer's condition as free from active tuberculosis. This certification is vital for the continuation of the volunteer's service within the school district, emphasizing the district's commitment to public health and safety. By requiring a signature from both the examining physician or surgeon and the school nurse, the form attests to the thoroughness of the health screening process, ensuring that all volunteers engage in their roles without posing health risks to themselves or others. This carefully structured process underscores the district's dedication to maintaining a safe educational environment, leveraging health documentation to prevent the spread of tuberculosis within its community.
| Question | Answer |
|---|---|
| Form Name | San Diego Tb Test Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | TUBERCULOSIS, INTRADERMAL, san diego tuberculin card, san diego district tuberculin card |
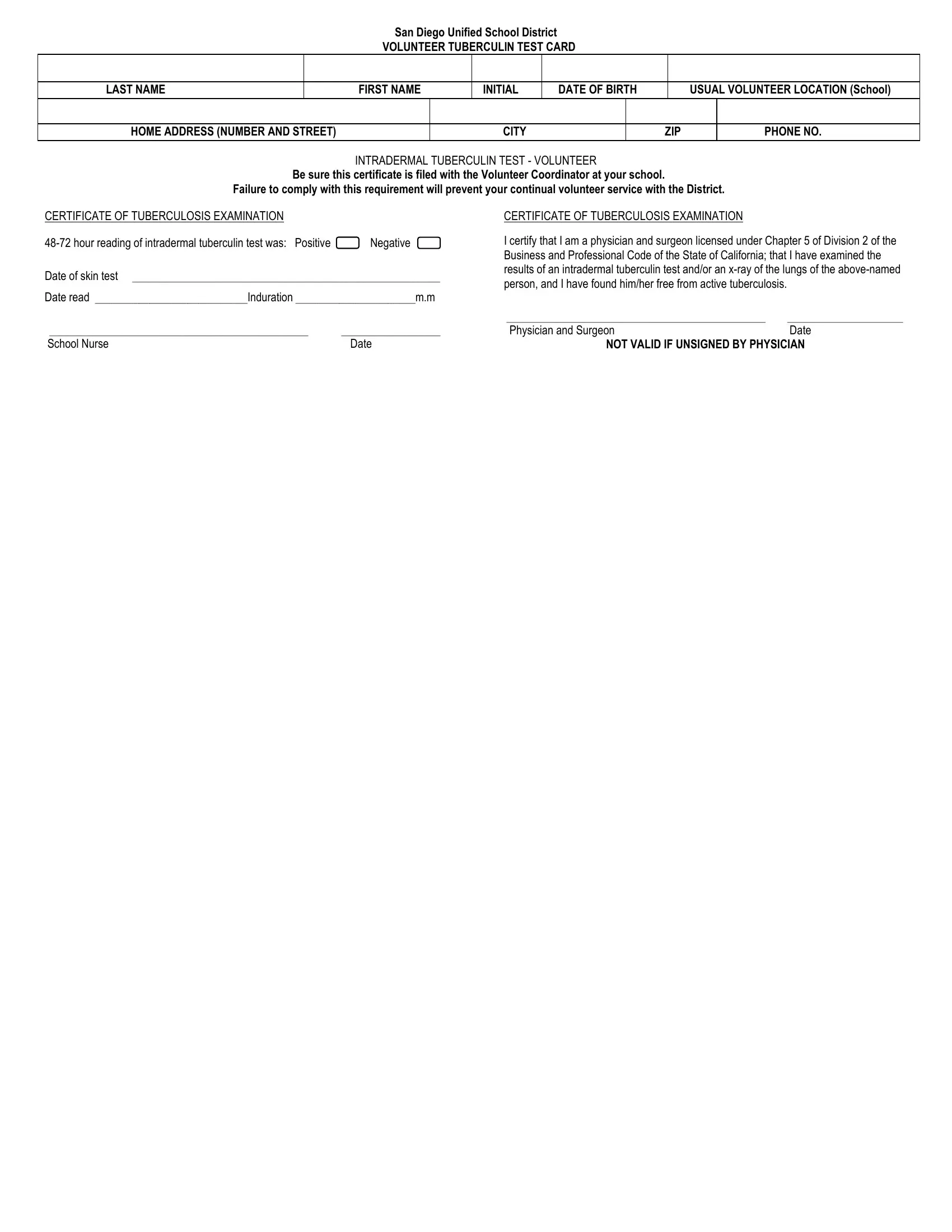
San Diego Unified School District
VOLUNTEER TUBERCULIN TEST CARD
LAST NAME
FIRST NAME
INITIAL
DATE OF BIRTH
USUAL VOLUNTEER LOCATION (School)
HOME ADDRESS (NUMBER AND STREET)
CITY
ZIP
PHONE NO.
INTRADERMAL TUBERCULIN TEST - VOLUNTEER
Be sure this certificate is filed with the Volunteer Coordinator at your school.
Failure to comply with this requirement will prevent your continual volunteer service with the District.
CERTIFICATE OF TUBERCULOSIS EXAMINATION
Date of skin test ________________________________________________________
Date read ____________________________Induration ______________________m.m
CERTIFICATE OF TUBERCULOSIS EXAMINATION
I certify that I am a physician and surgeon licensed under Chapter 5 of Division 2 of the Business and Professional Code of the State of California; that I have examined the results of an intradermal tuberculin test and/or an
_______________________________________________ _____________________
_______________________________________________ |
__________________ |
Physician and Surgeon |
Date |
School Nurse |
Date |
NOT VALID IF UNSIGNED BY PHYSICIAN |
|