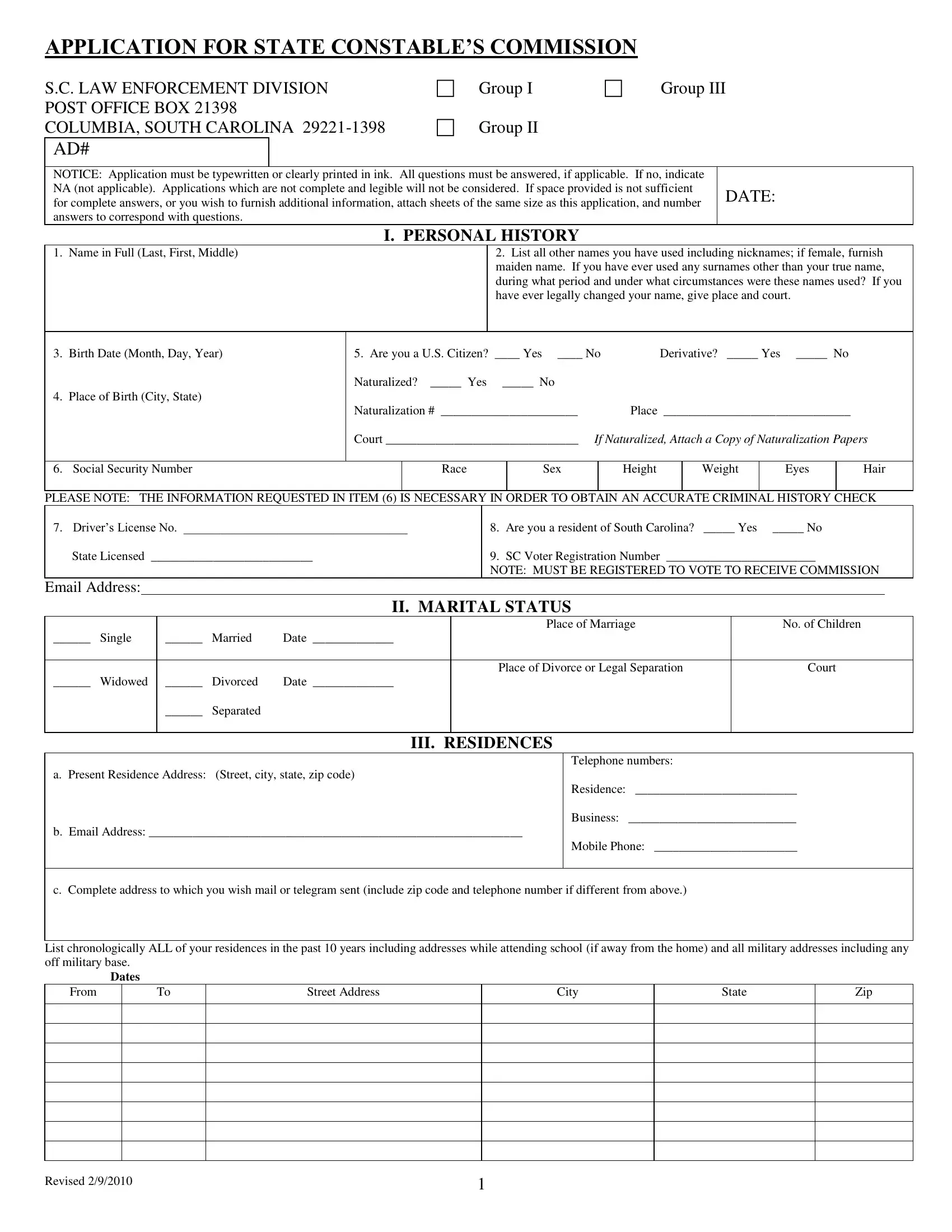
Embarking on the journey to become a South Carolina State Constable is a path filled with many steps, one of which is the completion of the State Constable's Commission Application. Managed by the South Carolina Law Enforcement Division, this application process is meticulous, requiring potential candidates to provide in-depth personal, educational, and professional information. The form divides into numerous sections, addressing personal history, education, a thorough employment history, and even detailed questions regarding marital status, residences, and any military service. Applicants are further queried on their financial status, any court records that may exist, including arrests or charges, and personal declarations about drug use or affiliations with organizations that are inimical to U.S. interests. The necessity for accuracy and completeness cannot be overstated, as omissions or errors can impact an applicant's consideration. Additionally, this comprehensive document seeks to evaluate the character and capabilities of individuals applying to serve as constables, ensuring they meet the high standards set forth for law enforcement personnel in South Carolina.
| Question | Answer |
|---|---|
| Form Name | Sc Application State Constable Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | application constable commission form, application constable commission online, south carolina application constable, sc real id application form |
APPLICATION FOR STATE CONSTABLE’S COMMISSION
S.C. LAW ENFORCEMENT DIVISION |
|
Group I |
|
Group III |
|
|
|
|
|||||||||||||||||
POST OFFICE BOX 21398 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
COLUMBIA, SOUTH CAROLINA |
|
Group II |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
AD# |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
NOTICE: Application must be typewritten or clearly printed in ink. All questions must be answered, if applicable. If no, indicate |
|
|
|
|
|
|
|
||||||||||||||||||
NA (not applicable). Applications which are not complete and legible will not be considered. If space provided is not sufficient |
|
DATE: |
|
|
|
|
|||||||||||||||||||
for complete answers, or you wish to furnish additional information, attach sheets of the same size as this application, and number |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||
answers to correspond with questions. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
I. PERSONAL HISTORY |
|
|
|
|
|
|
|
|
|
|
|
||||||||
1. Name in Full (Last, First, Middle) |
|
|
|
|
|
|
|
2. List all other names you have used including nicknames; if female, furnish |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
maiden name. If you have ever used any surnames other than your true name, |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
during what period and under what circumstances were these names used? If you |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
have ever legally changed your name, give place and court. |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
3. Birth Date (Month, Day, Year) |
|
5. Are you a U.S. Citizen? ____ Yes ____ No |
|
Derivative? _____ Yes |
_____ No |
|
|
||||||||||||||||||
|
|
|
|
|
|
Naturalized? |
_____ Yes _____ No |
|
|
|
|
|
|
|
|
|
|
|
|||||||
4. Place of Birth (City, State) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
Naturalization # ______________________ |
|
Place ______________________________ |
|
|
|||||||||||||||
|
|
|
|
|
|
Court _______________________________ If Naturalized, Attach a Copy of Naturalization Papers |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
6. Social Security Number |
|
|
|
|
Race |
|
|
|
Sex |
|
|
Height |
|
Weight |
|
Eyes |
|
Hair |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
PLEASE NOTE: THE INFORMATION REQUESTED IN ITEM (6) IS NECESSARY IN ORDER TO OBTAIN AN ACCURATE CRIMINAL HISTORY CHECK |
|||||||||||||||||||||||||
7. Driver’s License No. ____________________________________ |
|
|
|
|
8. Are you a resident of South Carolina? |
_____ Yes _____ No |
|
|
|||||||||||||||||
State Licensed __________________________ |
|
|
|
|
9. SC Voter Registration Number ________________________ |
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
NOTE: MUST BE REGISTERED TO VOTE TO RECEIVE COMMISSION |
|||||||||||||
Email Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
II. MARITAL STATUS |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Place of Marriage |
|
|
|
|
No. of Children |
|
|
|||||
______ |
Single |
______ |
Married |
Date _____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Place of Divorce or Legal Separation |
|
|
|
|
Court |
|
|
||||||
______ |
Widowed |
______ |
Divorced |
Date _____________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
______ |
Separated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. RESIDENCES
a.Present Residence Address: (Street, city, state, zip code)
b.Email Address: ____________________________________________________________
Telephone numbers:
Residence: __________________________
Business: ___________________________
Mobile Phone: _______________________
c. Complete address to which you wish mail or telegram sent (include zip code and telephone number if different from above.)
List chronologically ALL of your residences in the past 10 years including addresses while attending school (if away from the home) and all military addresses including any off military base.
|
Dates |
|
|
|
|
From |
To |
Street Address |
City |
State |
Zip |
Revised 2/9/2010 |
1 |
IV. EDUCATION
Calendar Years Attended
|
|
|
|
|
Circle Last |
Major Course |
Did You |
If Yes, Certificate or |
||
|
Name and Location |
From |
To |
|
Year Completed |
Of Study |
Graduate |
Degree Received |
||
High School |
|
|
|
9 |
10 |
11 |
12 |
|
|
|
College |
|
|
|
1 |
2 |
3 |
4 |
|
|
|
Graduate |
|
|
|
|
|
|
|
|
|
|
School |
|
|
|
1 |
2 |
3 |
4 |
|
|
|
Technical |
|
|
|
|
|
|
|
|
|
|
School |
|
|
|
1 |
2 |
3 |
4 |
|
|
|
Other |
|
|
|
1 |
2 |
3 |
4 |
|
|
|
|
|
|
Specialized Schools |
|
|
|
|
|||
Name and Address of School
Study or Specialization
From
To
4. Were you ever dismissed from a school, or was any disciplinary action ever taken against you during your scholastic career? ___ Yes |
___ No |
||||
|
|
|
|
|
|
School |
|
|
Date |
Action |
|
|
V. EMPLOYMENT HISTORY |
|
|||
NOTE: LIST LAST POSITION FIRST. Include chronological history of employment starting with current or most recent position. Account for all periods including casual employment and all periods of unemployment. Be sure to include military experience, if applicable. A resume of your employment will not be accepted in lieu of this information. Attach additional sheets as needed.
I.PRESENT OR LAST EMPLOYMENT (GIVE COMPLETE MAILING ADDRESSES AND ZIP CODES)
Employer ___________________________________________________________ Immediate Supervisor __________________________________________________
Employer’s Address (Street, City, State, Zip) ______________________________________________________________________________________________________
Telephone No. ______________________________ Date Employed _____________________________ Date Separated _______________________________
Job Title/Work Description __________________________________________ Starting Salary ___________________ Ending Salary ____________________________
Reason for Leaving ___________________________________________________________________________________________________________________________
II. PREVIOUS EMPLOYMENT
Employer ___________________________________________________________ Immediate Supervisor __________________________________________________
Employer’s Address (Street, City, State, Zip) ______________________________________________________________________________________________________
Telephone No. ______________________________ Date Employed _____________________________ Date Separated _______________________________
Job Title/Work Description __________________________________________ Starting Salary ___________________ Ending Salary ____________________________
Reason for Leaving ___________________________________________________________________________________________________________________________
III. PREVIOUS EMPLOYMENT
Employer ___________________________________________________________ Immediate Supervisor __________________________________________________
Employer’s Address (Street, City, State, Zip) ______________________________________________________________________________________________________
Telephone No. ______________________________ Date Employed _____________________________ Date Separated _______________________________
Job Title/Work Description __________________________________________ Starting Salary ___________________ Ending Salary ____________________________
Reason for Leaving ___________________________________________________________________________________________________________________________
IV. PREVIOUS EMPLOYMENT
Employer ___________________________________________________________ Immediate Supervisor __________________________________________________
Employer’s Address (Street, City, State, Zip) ______________________________________________________________________________________________________
Telephone No. ______________________________ Date Employed _____________________________ Date Separated _______________________________
Job Title/Work Description __________________________________________ Starting Salary ___________________ Ending Salary ____________________________
Reason for Leaving ___________________________________________________________________________________________________________________________
Have you ever been dismissed or asked to resign from any employment or position you have held? _____ Yes |
______ No If your answer is “Yes”, set forth your |
|
explanations on an attached sheet indicating the name of the company, your dates of employment and the reason(s) for your dismissal/resignation. |
||
Revised 2/9/2010 |
2 |
|
VI. MILITARY RECORDS
1. |
Are you registered for Selective Service? ___ Yes |
___ No Location: City and State _______________________________________________________ |
||||||
2. |
Have you ever served on active duty in the Armed Forces of the United States? ______ Yes |
______ No |
||||||
3. |
Branch of Military Service _____________________________________________ |
Type of Discharge __________________________ Basis ___________________ |
||||||
4. |
Dates of Active duty (month, day, year) From __________________ To __________________ |
5. Serial Number ________________________________________ |
||||||
6. |
Member of Reserve? ___ Yes ___ No |
|
Ready |
|
Standby |
Branch of Service ________________________ 7. Was any type of disciplinary action taken in the |
||
service? Be sure to include |
Details _____________________________________________________________ |
|||||||
8. |
National Guard: ___ Present ___ Former |
___ None. If you are a drilling member of the N.G., give name of unit & location __________________________________ |
||||||
|
|
|
|
|
|
VII. REFERENCES |
|
|
Give three references (not relatives, former or present employers, fellow employees or school teachers) who are responsible adults of reputable standing in their communities, such as property owners, business or professional men or women including your physician, if you have one, who have known you well for at least five years, preferably those who have known you during the past five years. If retired, give former occupation.
Complete Name _______________________________________________________________________ Years Known _________________________________________
Home Phone ______________________________________ Business Phone _______________________________________ Occupation ________________________
Home Address _______________________________________________________________________________________________________________________________
Business Address _____________________________________________________________________________________________________________________________
Complete Name _______________________________________________________________________ Years Known _________________________________________
Home Phone ______________________________________ Business Phone _______________________________________ Occupation ________________________
Home Address _______________________________________________________________________________________________________________________________
Business Address _____________________________________________________________________________________________________________________________
Complete Name _______________________________________________________________________ Years Known _________________________________________
Home Phone ______________________________________ Business Phone _______________________________________ Occupation ________________________
Home Address _______________________________________________________________________________________________________________________________
Business Address _____________________________________________________________________________________________________________________________
VIII. FOREIGN TRAVEL – (MILITARY SERVICE, RESIDENCE, VISIT)
1. Have you ever visited or resided in any foreign country (including travel in the Armed Forces of the U.S.)? ___ Yes ___ No Passport Number _________________________________ Date/Place Issued _____________________________________________
Country Visited
From
Month/Yr
To
Month/Yr
Reason for Travel
IX. COURT RECORD
1. Have you ever been arrested or charged with any violation including traffic, but excluding parking tickets? ____ Yes ____ No. To your knowledge, has any member of
your immediate family ever been convicted of any offense other than traffic violations? ____ Yes ____ No. If so, list all such matters even if not formally charged or no
court appearance, or found not guilty, or matter settled by payment of fine or forfeiture of collateral. Note: An affirmative answer will not necessarily disqualify you from consideration.
Date |
Place and Department |
Charge |
Court and Place |
Disposition |
Details |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relatives Name |
Place and Department |
Date/Charge |
Court and Place |
Disposition |
Details |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revised 2/9/2010 |
|
|
3 |
|
|

2. Have you ever been a plaintiff or defendant in a court action? ____ Yes ____ No. If so, give date, place, court, names of parties involved, nature of action, and final
disposition. NOTE: An affirmative answer will not necessarily disqualify you from consideration.
X. FINANCIAL STATUS
1. |
Do you have any sources of income other than your salary or that of your spouse? ___ Yes ___ No |
|
||||
|
If “Yes”, identify source and the amount that you receive from each such source. _______________________________________________________________________ |
|||||
2. |
Are you indebted to anyone? ___ Yes |
___ No (Note: List any debt over $100. |
Be sure to indicate student loans and charge accounts. Also list any debt, regardless of the |
|||
amount, where payment is past due.) |
|
|
|
|
|
|
|
Creditor |
|
Address |
|
Amount |
Loan or Account Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Have you ever been in or petitioned for bankruptcy? ___ Yes ___ No
If your answer is “Yes” to the above, give particulars, including court/date. _________________________________________________________________________
XI. SPECIAL QUALIFICATIONS AND SKILLS
1. Do you have foreign language ability? ____ |
Yes ____ No. |
If “Yes”, indicate your proficiency in each phase of each foreign language, listed as “Slight”, “Good”, or |
||||
“Fluent”. |
|
|
|
|
|
|
Name of Language |
|
Speak |
|
Understand |
Read |
Write |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Are you a member of the bar? ___ Yes ___ No Date _______________ |
State(s) _______________________ |
3. Are you a CPA? ___ Yes ___ No |
Date ________________ State(s) ________________________ |
4. Are you a licensed aircraft pilot? ___ |
Yes ___ No Rating(s) _____________ |
XII. |
RELATIVES |
|
All applicants must give complete information concerning their relatives. If you have been married more than once, give the requested information concerning each former husband or wife. Even though a parent is deceased, give all the information requested, and indicate last residence and year of death. Include stepbrothers and sisters, half brothers and sisters. If you have
FATHER: Last, First, Middle Name _____________________________________________________________________________________________________________
Address ________________________________________________________________ Occupation ________________________________________________________
Name & Address of Employer __________________________________________________________________________________________________________________
MOTHER: Last, First, Middle Name ____________________________________________________________________________________________________________
Address ________________________________________________________________ Occupation ________________________________________________________
Name & Address of Employer __________________________________________________________________________________________________________________
SPOUSE: Last, First, Middle Name _____________________________________________________________________________________________________________
Address ________________________________________________________________ Occupation ________________________________________________________
Name & Address of Employer __________________________________________________________________________________________________________________
Birth Date _____________________________________________________ Place of Birth _______________________________________________________________
FORMER SPOUSE: Last, First, Middle Name ____________________________________________________________________________________________________
Address ________________________________________________________________ Occupation ________________________________________________________
Name & Address of Employer __________________________________________________________________________________________________________________
Birth Date _____________________________________________________ Place of Birth _______________________________________________________________
CHILDREN (List names and ages) _____________________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________________
BROTHERS/SISTERS (List names and ages) _____________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________________
OTHER INDIVIDUALS WITH WHOM YOU HAVE RESIDED OVER A PERIOD OF 30 DAYS OR MORE: Indicate relationship. Include roommates for the last five years only.
Last, First, Middle Name _______________________________________________________________________________________________________________________
Address ________________________________________________________________ Occupation ________________________________________________________
Revised 2/9/2010 |
4 |
Name & Address of Employer __________________________________________________________________________________________________________________
Birth Date _____________________________________________________ Place of Birth _______________________________________________________________
XIII. RELATIVES EMPLOYED BY THE STATE OR FEDERAL GOVERNMENT
List the complete names of any of your close relatives (including |
|
||
Complete Name |
Relationship |
Agency by Which Employed |
Location |
XIV. FRIENDS OR ACQUAINTANCES EMPLOYED BY THE STATE OR FEDERAL GOVERNMENT
Complete Name
Location
Length of Acquaintance
XV. PHYSICAL DATA
1. |
Do you now have or have you ever had any of the following: nervous; mental or emotional disorder of any sort; hypertension; tuberculosis; epilepsy; fainting spells or |
||||||||
|
severe headaches; diabetes; ulcers; rheumatic fever or heart disease; or asthma? ____ Yes ____ |
No. If “Yes”, describe, giving date(s) of illness(es), attending physician, |
|||||||
|
and hospital or institution where treated (if applicable). |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
||
2. |
Do you now have or have you ever had any chronic or serious illnesses; or have you ever had any serious operations or injuries? ____ Yes |
____ No. If “Yes”, describe, |
|||||||
|
giving date(s) of illness(es), or operation(s), attending physician, and hospital or institution where treated (if applicable). |
|
|||||||
|
|
From Month/Yr |
To Month/Yr |
|
Hospital |
|
Location |
|
Reason |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. Describe any past or present physical handicap, or disability, not previously covered, but including extent of defective vision, if any, with and without glasses and deficiencies in color vision and hearing. Have you ever undergone radial keratonomy? ____ Yes ____ No. If “Yes”, give date(s), attending physician(s) and location(s)
where procedure was performed.
Corrected |
20/_____________________ |
Corrected |
20/_____________________ |
RIGHT EYE |
|
LEFT EYE |
|
Uncorrected |
20/_____________________ |
Uncorrected |
20/_____________________ |
4. Have you ever received, is there pending, have you applied for, or do you intend to apply for pension or compensation for any disability? ____ Yes ____ No. If “Yes”,
specify what kind, granted by whom, and what amount, when, why. If applicable, include Veteran’s Administration claim number.
____________________________________________________________________________________________________________________________________________
5. Do you have any physical defects such as, but nor limited to, a bone, joint or other deformity or loss of finger, which would preclude unrestricted, regular participation in all phases of firearms training, physical training and defensive tactics? ____ Yes ____ No. If “Yes”, describe:
____________________________________________________________________________________________________________________________________________
Note: An affirmative answer to any or all questions
XVI. PERSONAL DECLARATIONS
1. Do you use or have you ever used intoxicants? ____ Yes ____ No. 2. If so, to what extent? ___________________________________________________________
____________________________________________________________________________________________________________________________________________
3. Do you use or have you ever used such items as marijuana, hashish, cocaine, LSD, amphetamines, heroin, or drugs of a similar nature? ____ Yes ____ No.
____________________________________________________________________________________________________________________________________________
4. If answer to Question 3 above is “Yes”, complete the following items for each drug used: |
|
||||
a. Drug |
|
|
b. How taken |
|
_____ |
c. Circumstances _________________________ |
d. How many times used __________________ e. First time used __________ f. Last time used _____________ |
||||
____________________________________________________________________________________________________________________________________________
5. List the names of all federal, state or local government departments, agencies, or offices (including law enforcement) to which you have applied for employment.
____________________________________________________________________________________________________________________________________________
6. If to your knowledge any of the above have conducted an investigation of you, indicate the name of the agency and the approximate date of the investigation.
____________________________________________________________________________________________________________________________________________
7.Are you now or have you ever been a member of any foreign or domestic organization, association, movement, group or combination of persons which is totalitarian, fascist, communist, or subversive or which has adopted, or shows a policy of advocating or approving the commission of acts of force or violence to deny other persons their
rights under the Constitution of the United States, or which seeks to alter the form of government of the U.S. by unconstitutional means? ____ Yes ____ No. (If answer to
any of these is “Yes”, explain fully.)
____________________________________________________________________________________________________________________________________________
8. Do you or any member of your immediate family engage in employment or take an active part in the management, direction or operation of any business, trade or profession or have any financial interest in any business, trade or profession which might pose a conflict of interest with your being a State Constable? ____ Yes ____ No.
(If answer to any of these is “Yes”, explain fully.)
____________________________________________________________________________________________________________________________________________
Revised 2/9/2010 |
5 |
9. An investigation will be conducted of all information listed on this application. Because of this, are you aware of any information about yourself or any person with whom
you are or have been closely associated (including relatives and roommates) which might tend to reflect unfavorably on your reputation, morals, character, ability or loyalty to the United States? ____ Yes ____ No. If “Yes”, please attach a separate piece of paper, appropriately numbered, giving your version of this/these incident(s).
____________________________________________________________________________________________________________________________________________
10. Have you previously applied for or held a State Constable’s Commission? ____ Yes ____ No. If yes, give date_____________________________________________
____________________________________________________________________________________________________________________________________________
XVI. PERSONAL DECLARATIONS (CONT’D)
11. If appointed as a State Constable, are you willing to assist any law enforcement agency in South Carolina if called upon to do so? ____ Yes ____ No.
____________________________________________________________________________________________________________________________________________
12. Have you ever applied for or received any other type of law enforcement commission? ____ Yes ____ No. If “Yes”, give dates and details _____________________
____________________________________________________________________________________________________________________________________________
13. Do you currently hold any elected or appointed government position? ____ Yes ____ No. If “Yes”, state position __________________________________________
____________________________________________________________________________________________________________________________________________
14. Have you had any prior law enforcement training? ____ Yes ____ No. If “Yes”, give type of training, date, location and duration _____________________________
____________________________________________________________________________________________________________________________________________
15. Are you currently involved in any private security and/or private detective work? ____ Yes ____ No. If “Yes”, give details ___________________________________
____________________________________________________________________________________________________________________________________________
16. Do you currently have a financial interest in any private security and/or private detective agency? ____ Yes ____ No. If “Yes”, give name of company and state your
interest, stockholder, etc. _______________________________________________________________________________________________________________________
____________________________________________________________________________________________________________________________________________
17. Are you currently employed by a county or municipal government agency?____________________________________________________________________________
(a) |
Name of Agency |
Position |
____________________________________________________________ |
__________________________________________________________________ |
|
____________________________________________________________ |
__________________________________________________________________ |
|
____________________________________________________________________________________________________________________________________________
(b) Do you intend to use a State Commission, if approved, in your capacity within county or municipal government? ____ Yes ____ No.
____________________________________________________________________________________________________________________________________________
ALL APPLICANTS: A Group III state constable commission is issued for the sole purpose of enabling a citizen who has the proper training to volunteer assistance to requesting law enforcement departments when specifically approved by SLED.
State constable commissions are not issued to merely enable a citizen to carry firearms or to engage in independent law enforcement activity.
Approval of this application requires that you have made arrangements to assist the police and sheriff’s departments listed herein and that the chief of police or sheriff has requested your assistance.
____________________________________________________________________________________________________________________________________________
LIST THE POLICE AND SHERIFF’S DEPARTMENTS YOU HAVE ARRANGED TO ASSIST:
Police Chief/Sheriff
Telephone #
THIS STATEMENT MUST BE SIGNED
My signature hereon certifies my understanding and agreement that appointment as a state constable is without compensation from the State of South Carolina or any law enforcement department, that my commission may be revoked at the pleasure of the Governor, and that the application fee is
I certify my understanding and agreement that any appointment tendered me will be contingent upon the results of a character and fitness investigation and that withholding or submitting inaccurate information in this application package is a basis for denial of this application or revocation of my state constable commission if discovered later.
I certify my understanding and agreement that I will be participating with police officers in law enforcement training and patrol and other activities that might be strenuous and dangerous.
I certify my understanding and agreement that if I am commissioned as a Group III state constable, I will not be insured for personal injuries I might sustain or for
liability arising from my actions unless the following circumstances are true: (1) I am assisting a law enforcement department that has written to SLED requesting my assistance; (2) the department has certified to SLED that I am insured by the department’s worker’s compensation and liability insurance plans; (3) SLED has approved the department’s request in writing.
I certify that all information submitted on this form and accompanying documents is true and complete.
_____
Date |
Signature |
Revised 2/9/2010 |
6 |