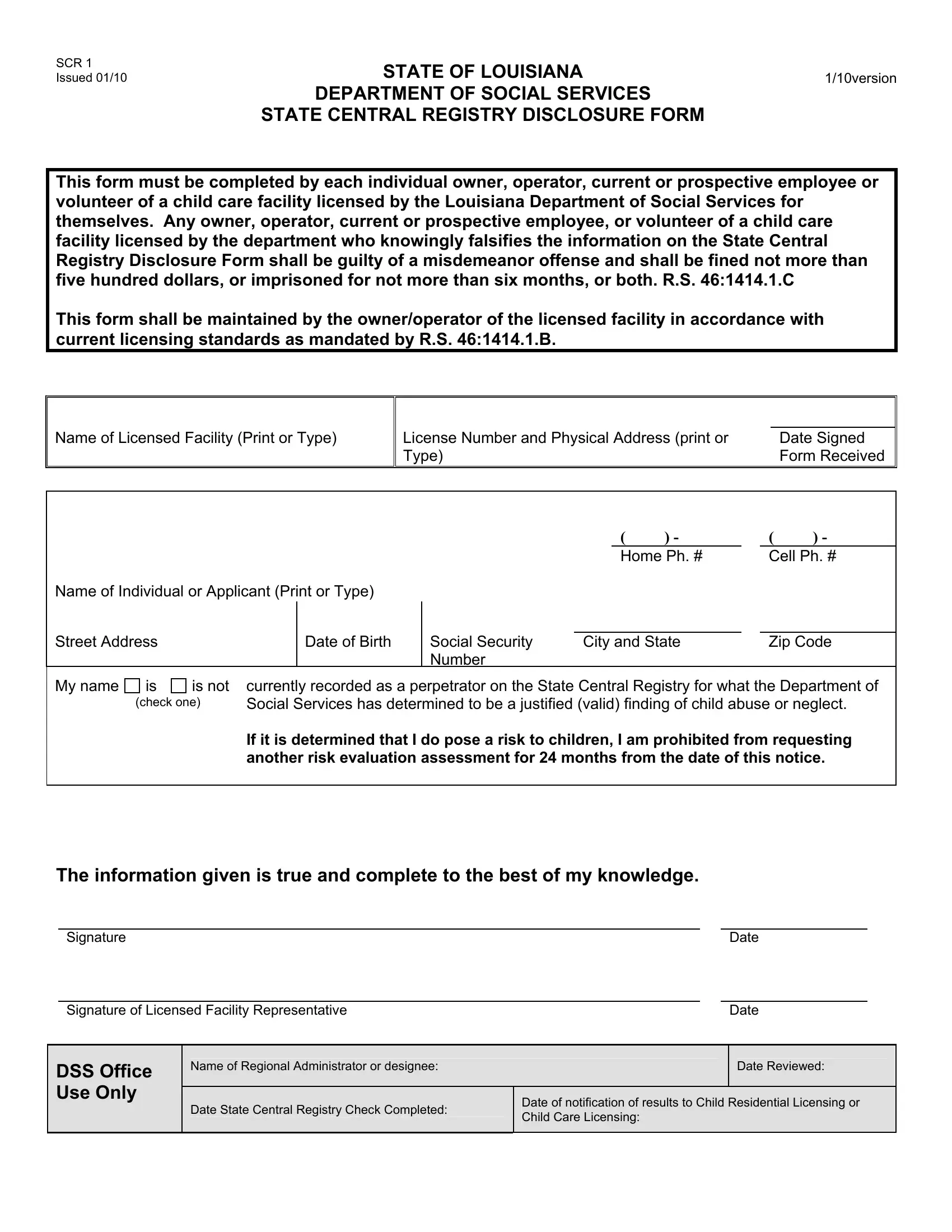
The SCR 1 form is an essential document that must be completed by individuals associated with child care facilities in Louisiana, including owners, operators, and anyone looking to work or volunteer at such establishments. Designed to ensure the safety and well-being of children, this form serves as a disclosure to the Louisiana Department of Social Services, verifying whether an individual has been recorded as a perpetrator of child abuse or neglect. Given the gravity of this responsibility, falsifying information on this form is considered a misdemeanor offense, inviting fines up to five hundred dollars, imprisonment for up to six months, or both. This strict enforcement underscores the commitment of the state to maintain the highest standards of care in child care facilities. The process of completing the form involves providing detailed personal information, affirming the absence or presence of a record in the State Central Registry for child abuse or neglect, and if flagged as a risk, facing restrictions on reevaluation for 24 months. Maintaining this form according to current licensing standards is mandated by the department, emphasizing the careful balance between legal compliance and the overarching goal of protecting children in child care environments.
| Question | Answer |
|---|---|
| Form Name | Scr 1 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Applicant, louisiana state registry form, mandated, SCR |
SCR 1 Issued 01/10
STATE OF LOUISIANA |
1/10version |
|
|
DEPARTMENT OF SOCIAL SERVICES |
|
STATE CENTRAL REGISTRY DISCLOSURE FORM |
|
This form must be completed by each individual owner, operator, current or prospective employee or volunteer of a child care facility licensed by the Louisiana Department of Social Services for themselves. Any owner, operator, current or prospective employee, or volunteer of a child care facility licensed by the department who knowingly falsifies the information on the State Central Registry Disclosure Form shall be guilty of a misdemeanor offense and shall be fined not more than five hundred dollars, or imprisoned for not more than six months, or both. R.S. 46:1414.1.C
This form shall be maintained by the owner/operator of the licensed facility in accordance with current licensing standards as mandated by R.S. 46:1414.1.B.
Name of Licensed Facility (Print or Type)
|
|
License Number and Physical Address (print or |
Date Signed |
Type) |
Form Received |
Name of Individual or Applicant (Print or Type)
Street Address |
Date of Birth |
|
|
( |
) - |
( |
) - |
|
Home Ph. # |
|
Cell Ph. # |
||
Social Security |
City and State |
Zip Code |
Number |
|
|
My name
is |
is not |
currently recorded as a perpetrator on the State Central Registry for what the Department of |
(check one) |
Social Services has determined to be a justified (valid) finding of child abuse or neglect. |
|
If it is determined that I do pose a risk to children, I am prohibited from requesting another risk evaluation assessment for 24 months from the date of this notice.
The information given is true and complete to the best of my knowledge.
Signature |
|
Date |
|
|
|
Signature of Licensed Facility Representative |
|
Date |
DSS Office Use Only
Name of Regional Administrator or designee:
Date State Central Registry Check Completed:
Date Reviewed:
Date of notification of results to Child Residential Licensing or Child Care Licensing: