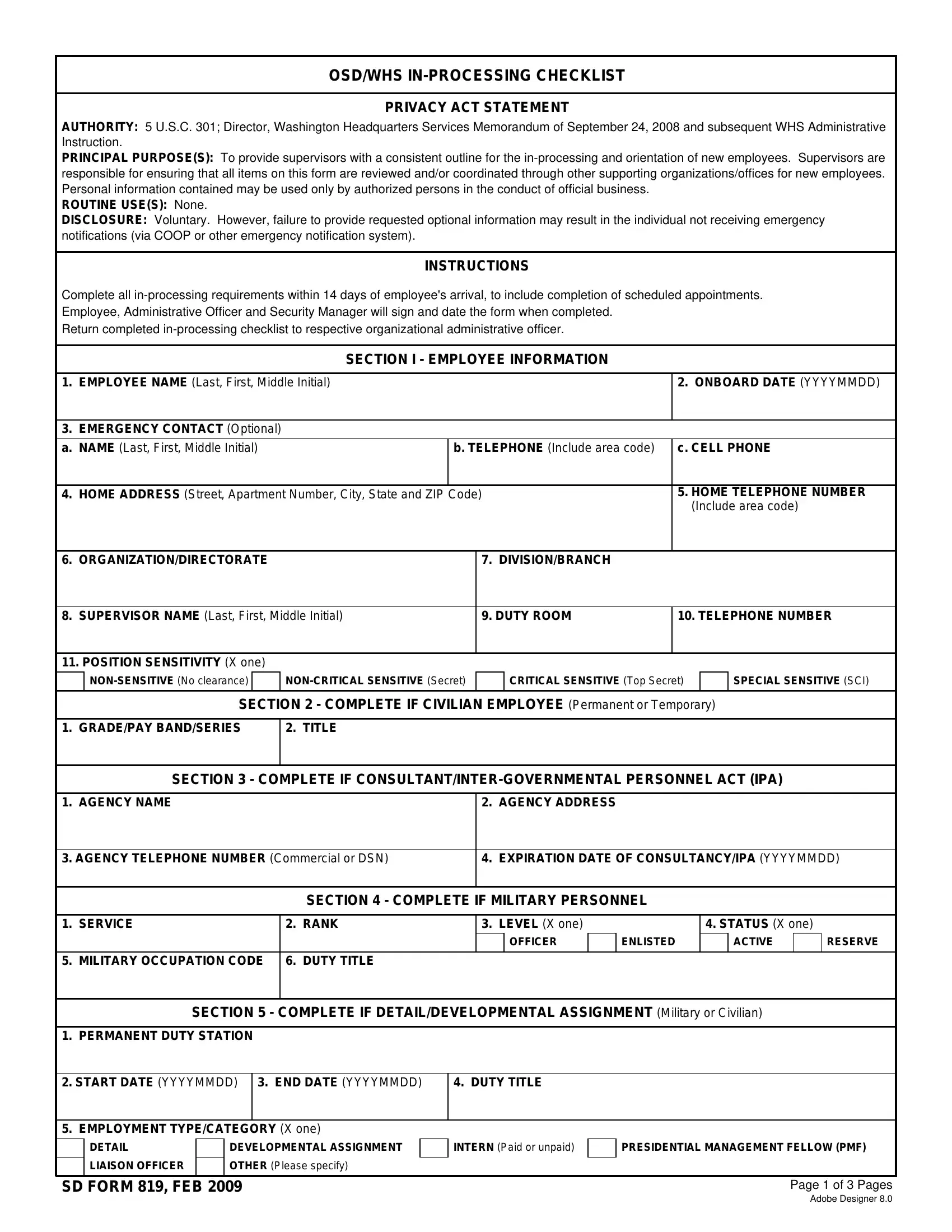
In the intricate fabric of governmental operations, the SD Form 819 emerges as a critical document designed to streamline the in-processing and orientation of new employees within the Department of Defense's Office of the Secretary of Defense (OSD) and Washington Headquarters Services (WHS). This comprehensive checklist serves multiple functions—anchored by the authority of the Director, Washington Headquarters Services Memorandum from September 24, 2008, and subsequent administrative instructions. It aims to offer supervisors a uniform framework to ensure a thorough review and coordination of various procedural requirements for newcomers through different supporting organizations and offices. The form meticulously gathers personal details necessary for conducting official business, strictly accessible to authorized personnel, thereby underlining its role in safeguarding privacy. The essence of the checklist spans across emergency planning, physical security, information technology, and other areas vital for integrating an employee into the governmental workflow. The disclosure of information is voluntary, highlighting the balance between employee autonomy and organizational requirements. However, the form also clarises the potential impact of withholding information, such as affecting emergency notification measures. With specified timelines and the need for signatures from the employee, Administrative Officer, and Security Manager upon completion, the SD Form 819 encapsulates a vital procedural bridge for onboarding, reflecting the underlying bureaucratic and operational discipline characteristic of governmental bodies.
| Question | Answer |
|---|---|
| Form Name | Sd Form 819 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | sd0819 whs inprocessing checklist form |
OSD/WHS
PRIVACY ACT STATEMENT
AUTHORITY: 5 U.S.C. 301; Director, Washington Headquarters Services Memorandum of September 24, 2008 and subsequent WHS Administrative Instruction.
PRINCIPAL PURPOSE(S): To provide supervisors with a consistent outline for the
ROUTINE USE(S): None.
DISCLOSURE: Voluntary. However, failure to provide requested optional information may result in the individual not receiving emergency notifications (via COOP or other emergency notification system).
INSTRUCTIONS
Complete all
Return completed
SECTION I - EMPLOYEE INFORMATION
1. |
EMPLOYEE NAME (Last, First, Middle Initial) |
|
|
2. ONBOARD DATE (YYYYMMDD) |
|
|
|
|
|
3. |
EMERGENCY CONTACT (Optional) |
|
|
|
|
|
|
|
|
a. NAME (Last, First, Middle Initial) |
b. TELEPHONE (Include area code) |
c. CELL PHONE |
||
|
|
|
|
|
4. |
HOME ADDRESS (Street, Apartment Number, City, State and ZIP Code) |
5. HOME TELEPHONE NUMBER |
||
|
|
|
|
(Include area code) |
|
|
|
|
|
6. |
ORGANIZATION/DIRECTORATE |
|
7. DIVISION/BRANCH |
|
|
|
|
|
|
8. |
SUPERVISOR NAME (Last, First, Middle Initial) |
|
9. DUTY ROOM |
10. TELEPHONE NUMBER |
|
|
|
|
|
11. POSITION SENSITIVITY (X one) |
|
|
|
|
CRITICAL SENSITIVE (Top Secret)
SPECIAL SENSITIVE (SCI)
SECTION 2 - COMPLETE IF CIVILIAN EMPLOYEE (Permanent or Temporary)
1. GRADE/PAY BAND/SERIES
2. TITLE
SECTION 3 - COMPLETE IF
1. |
AGENCY NAME |
|
|
2. |
AGENCY ADDRESS |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||
3. AGENCY TELEPHONE NUMBER (Commercial or DSN) |
4. |
EXPIRATION DATE OF CONSULTANCY/IPA (YYYYMMDD) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 4 - COMPLETE IF MILITARY PERSONNEL |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
SERVICE |
2. |
RANK |
3. |
LEVEL (X one) |
|
4. STATUS (X one) |
|
||||
|
|
|
|
|
|
OFFICER |
|
ENLISTED |
|
ACTIVE |
|
RESERVE |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
MILITARY OCCUPATION CODE |
6. |
DUTY TITLE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 5 - COMPLETE IF DETAIL/DEVELOPMENTAL ASSIGNMENT (Military or Civilian)
1. PERMANENT DUTY STATION
2. START DATE (YYYYMMDD) |
3. END DATE (YYYYMMDD) |
4. DUTY TITLE |
|
|
|
5. EMPLOYMENT TYPE/CATEGORY (X one) |
|
|
DETAIL
LIAISON OFFICER
DEVELOPMENTAL ASSIGNMENT
OTHER (Please specify)
INTERN (Paid or unpaid)
PRESIDENTIAL MANAGEMENT FELLOW (PMF)
SD FORM 819, FEB 2009 |
Page 1 of 3 Pages |
Adobe Designer 8.0
SECTION 6 - COMPLETE IF CONTRACTOR PERSONNEL
1. COMPANY NAME |
2. COMPANY ADDRESS (Street, Suite No., City, State and ZIP Code) |
||
|
|
|
|
3. COMPANY TELEPHONE NUMBER (Include area code) |
4. EXPIRATION DATE OF CONTRACT (YYYYMMDD) |
||
|
|
|
|
|
SECTION 7 - |
||
|
|
|
|
Organizations should enter specific location/room numbers as appropriate. |
|
|
|
Enter "N/A" under "date completed" for inapplicable action items. |
|
|
|
|
|
|
|
|
ACTION ITEM |
|
INITIAL/DATE COMPLETED |
|
|
|
|
1. COMPONENT (OSD/WHS Component Administrative Officer) |
|
Room No.: |
|
|
|
|
|
a. Personnel Locator Form |
|
|
|
|
|
|
|
b. Update Organizational Telephone Directory |
|
|
|
|
|
|
|
c. Parking Information (Pentagon or PMI) |
|
|
|
|
|
|
|
d. NCR Mass Transit Subsidy Program |
|
|
|
|
|
|
|
e. Government Travel Credit Card |
|
|
|
|
|
|
|
f. |
Government Travel Card Account Transfer Form |
|
|
|
|
||
g. DD Form 2918 or SD Form 37 for financial disclosure filing determination |
|
||
|
|
|
|
h. Telephone set up and password |
|
|
|
|
|
|
|
i. Notification to Defense Travel System (DTS) Manager |
|
|
|
|
|
||
j. Issue Morale and Welfare (MWR) membership card for OSD Welfare and Recreation Association |
|
||
|
(civilian and military only) |
|
|
|
|
|
|
k. Provide information on Pentagon Library |
|
|
|
|
|
|
|
l. Provide information on Pentagon Athletic Center |
|
|
|
|
|
|
|
m. Obtain copy of Military Orders if applicable |
|
|
|
|
|
|
|
2. EMERGENCY PLANNING (COOP ADMINISTRATOR) |
|
Room No.: |
|
|
|
|
|
a. Escape Mask Equipment and Training |
|
|
|
|
|
|
|
b. Provide organization evacuation procedures and egress route map |
|
|
|
|
|
|
|
c. Add employee to Emergency Notification System (NOTIFIND) |
|
|
|
|
|
|
|
d. Issue Government Emergency Telephone System (GETS) card |
|
|
|
|
|
|
|
e. Update organizational COOP roster |
|
|
|
|
|
|
|
f. Add employee information to DFD Emergency Preparedness List |
|
|
|
|
|
|
|
g. Special badging requirements for COOP deployers |
|
|
|
|
|
|
|
h. Provide copy of |
|
|
|
|
|
|
|
3. MILITARY PERSONNEL |
|
Pentagon, Room 5E565 |
|
|
|
|
|
a. Military member check in with WHS/Military Personnel Services |
|
|
|
|
|
|
|
b. Provide copy of orders to organizational component |
|
|
|
|
|
|
|
4. PHYSICAL SECURITY |
|
Room No.: |
|
|
|
||
a. Provide Federal Employee Compensation Act (FECA) physical security reporting information |
|
||
|
(e.g., hazards, accidents, injuries, illnesses) |
|
|
|
|
||
b. Provide information on safety training, medical, personal protective equipment |
|
||
|
|
||
c. Provide ergonomic information and assessment of workstation for identifying accessibility needs |
|
||
|
if applicable |
|
|
|
|
|
|
SD FORM 819, FEB 2009 |
Page 2 of 3 Pages |

|
|
|
|
ACTION ITEM |
INITIAL/DATE COMPLETED |
|||
|
|
|
|
|
|
|
|
|
5. SECURITY MANAGER |
|
|
|
|
Room No.: |
|||
|
|
|
|
|
|
|
|
|
a. Identification Cards |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
(1) Common Access Card (CAC) - fingerprint requirement, NACI |
|
||||||
|
|
|
|
|
|
|
|
|
|
(2) NCR/Contractor Badge |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
b. Security notification for DoD civilians and military |
|
|
||||||
|
|
|
|
|
|
|
||
c. Security notification for contractors (Visit Authorization Request (VAR)) |
|
|||||||
|
|
|
|
|
|
|
|
|
d. Completion and signature on Standard Form 312 |
|
|
||||||
|
|
|
|
|
|
|
|
|
e. Attestation completed |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
f. |
Component Security Briefings as required |
|
|
|||||
|
|
|
|
|
|
|
|
|
g. Courier Card (if needed) |
|
|
|
|
|
|||
|
|
|
|
|
|
|
||
h. Security Access (Swipe Access/SIRP Access/Lan Room/PIC Numbers) |
|
|||||||
|
|
|
|
|
|
|
|
|
6. INFORMATION TECHNOLOGY |
|
|
|
|
Room No.: |
|||
|
|
|
|
|
|
|
||
a. Signed DD Form 2875, "System Authorization Access Request (SAAR)", to create account |
|
|||||||
|
(e.g., local and global email accounts) |
|
|
|||||
|
|
|
|
|
|
|
||
b. Request for IT Equipment, COOP IT Equipment (e.g., laptop, BlackBerry, cellular phone, |
|
|||||||
|
if needed) |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
c. Domain Manager Identification |
|
|
|
|
|
|||
|
|
|
|
|
|
|
||
d. Contact WHS Enterprise Service Desk - (703) |
|
|||||||
|
|
|
|
|
|
|
|
|
e. Read and sign "Consent to Monitor" Statement |
|
|
||||||
|
|
|
|
|
|
|
|
|
f. Create Remedy Account, if needed |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
g. IA Certification (X one) |
|
|
User |
|
|
System Administrator |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
h. Establish global email account |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
7. SUPERVISOR |
|
|
|
|
Room No.: |
|||
|
|
|
|
|
|
|
||
a. Notify timekeeper and/or add account authorization for ATAAPS |
|
|||||||
|
|
|
|
|
|
|
||
b. Identify system access needed and take appropriate action to initiate required paperwork |
|
|||||||
|
|
|
|
|
|
|
||
c. Office space secure lock combinations (e.g., cipher |
|
|||||||
|
|
|
|
|
|
|
||
d. IDS alarm access established; PIC/PIN provided to employee if applicable |
|
|||||||
|
|
|
|
|
|
|
||
e. Address NSPS responsibilities (performance plan, appropriate training) |
|
|||||||
|
|
|
|
|
|
|
||
f. Identify development and training plan as appropriate |
|
|||||||
|
|
|
|
|
|
|
||
g. Schedule orientation and mandatory/recommended training |
|
|||||||
|
|
|
|
|
|
|
|
|
h. Brief employee on MyBiz and MyPay accounts |
|
|
||||||
|
|
|
|
|
|
|
||
i. Office of General Counsel (OGC) Standards of Conduct (OGE Form 450 within 30 days), if |
|
|||||||
|
applicable |
|
|
|
|
|
||
|
|
|
|
|
|
|
||
j. Schedule in Brief with Organization Director if applicable |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION 8 - CERTIFICATIONS |
|
|
|
|
|
|
|
|||
1.a. EMPLOYEE SIGNATURE |
|
|
|
|
b. DATE SIGNED (YYYYMMDD) |
|||
|
|
|
|
|||||
2.a. ADMINISTRATIVE OFFICER SIGNATURE |
|
b. DATE SIGNED (YYYYMMDD) |
||||||
|
|
|
|
|||||
3.a. SECURITY MANAGER SIGNATURE |
|
b. DATE SIGNED (YYYYMMDD) |
||||||
|
|
|
|
|
|
|
|
|
SD FORM 819, FEB 2009
Reset
Page 3 of 3 Pages