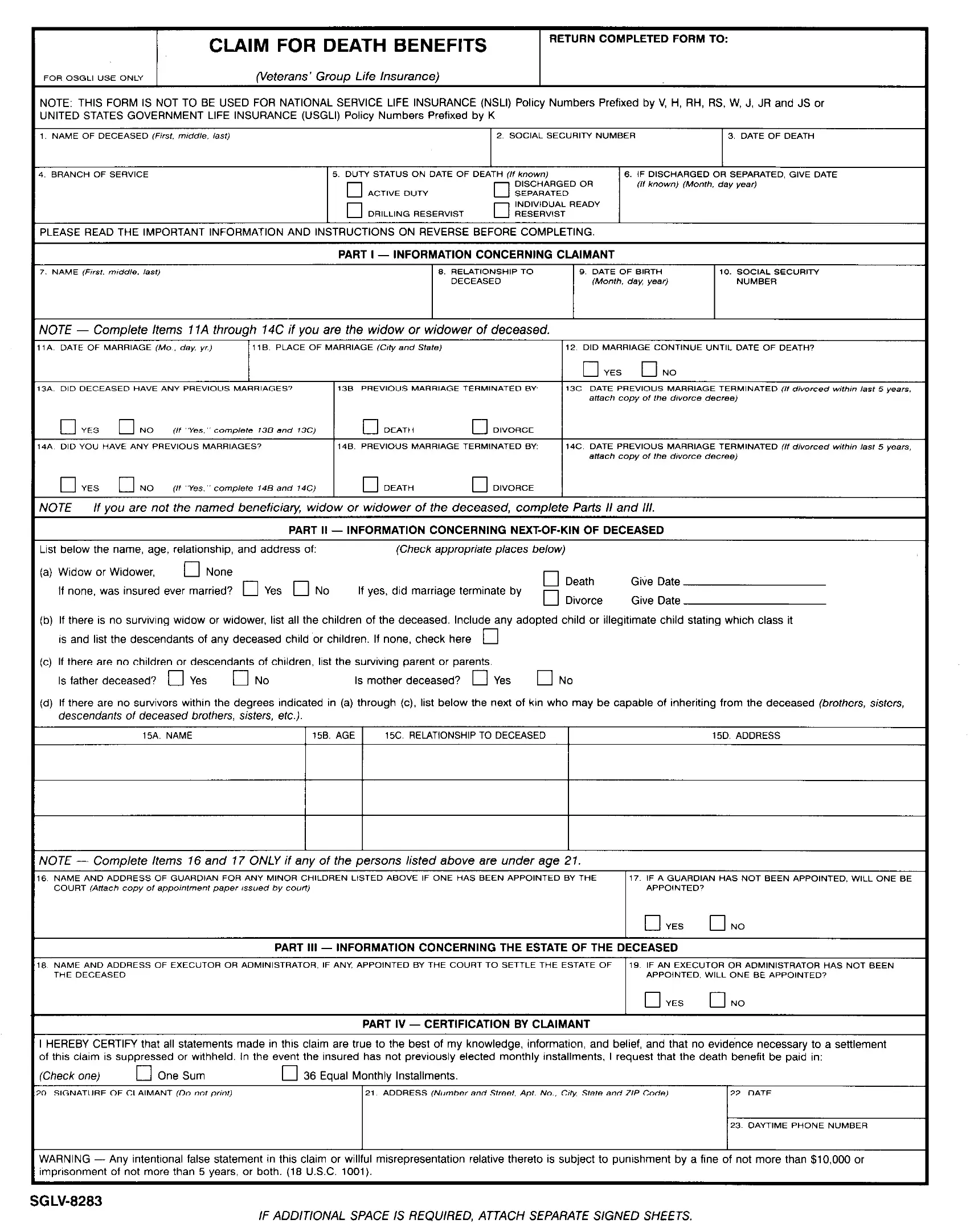
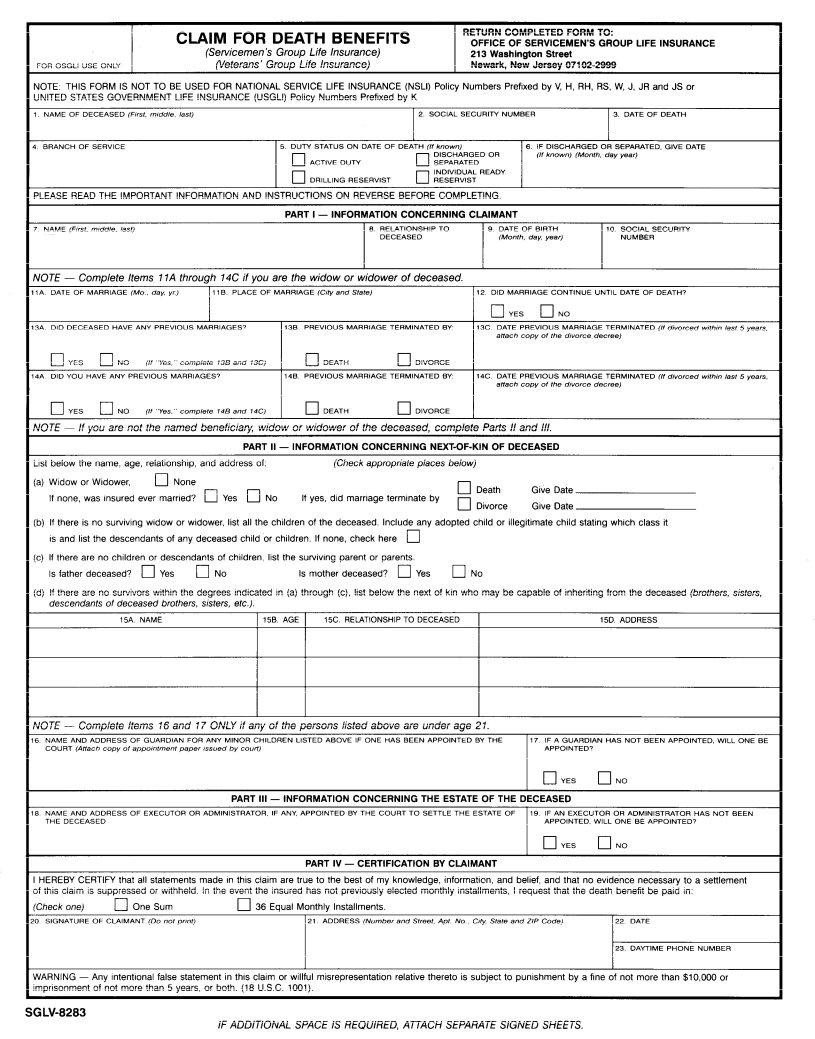
The SGLV 8283 form, known as the Claim for Death Benefits, plays a pivotal role for families navigating the challenging times following the loss of a loved one who served in the United States armed forces. Designed for beneficiaries under the Servicemen’s Group Life Insurance (SGLI) and Veterans’ Group Life Insurance (VGLI) policies, it sets the process in motion to secure vital financial support posthumously. The form clarifies it is not applicable for National Service Life Insurance or United States Government Life Insurance policies, marking a clear boundary on its applicability. Detailed instructions ensure claimants provide all necessary information, including the full name and Social Security number of the deceased, date and details of death, plus the claimant's relationship and identifying information. It emphasizes the importance of furnishing complete and accurate details to prevent delays in claim processing, with a caution against the submission of false information under penalty of law. For those who are primary beneficiaries, like spouses or children, as well as for those who might inherit in the absence of a named beneficiary, the document outlines a clear hierarchy of recipients, ensuring that the benefits reach the hands of those intended. With required evidence varying based on the deceased's service status at the time of death, the form also guides users on the necessary documentation to accompany claims, simplifying a process that can seem daunting during a period of grief.
| Question | Answer |
|---|---|
| Form Name | Sglv 8283 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 8283 form sglv, form 8283 sglv, sglv8283 form print, sglv 8283 forms |
CLAIM FOR DEATH BENEFITS
(Servicemen’s |
Group |
Life Insurance) |
|
|
|
|
|
(Veterans’ |
Group |
Life |
Insurance) |
\lOTE. THIS FORM IS NOT TO BE USED FOR NATIONAL SERVICE LIFE INSURANCE JNITED STATES GOVERNMENT LIFE INSURANCE (USGLI) Policy Numbers Prefixed
NAME OF DECEASED (FKS,, mrddle. /ast,
RETURN |
COMPLETED |
FORM |
TO: |
|||
|
OFFICE |
OF |
SERVICEMEN’SE |
|
INSURANCE |
|
|
Newark, |
New |
Jersey |
|
|
|
(NSLI) Policy Numbers Prefixed by V, H, RH, RS, W, J, JR and JS or by K
2 SOCIAL SECURITY NUMBER |
3. DATE OF DEATH |
‘LEASE READ THE IMPORTANT INFORMATION AND INSTRUCTIONS ON REVERSE BEFORE COMPLETING
PART I - INFORMATION CONCERNING CLAIMANT
VOTE - Comolete Items 11A throuah 14C if vou are the widow or widower of deceased.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
attach |
copy |
Of |
Ihe |
d,“orce |
decree, |
|
|
|
|
|
|
|
0 |
YES |
|
ON0 |
|
(,‘ |
“Yes. |
” complete |
|
148 |
and |
14c, |
|
|
|
cl |
|
DEATH |
|
|
|
cl |
|
DIVORCE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
VOTE |
- |
If vou |
are |
not |
the named |
beneficiarv. |
widow |
|
or |
widower |
of |
the |
deceased, |
|
comolete |
Parts |
II |
and |
III. |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
PART |
II - |
|
INFORMATION |
CONCERNING |
|
|
OF |
DECEASED |
|
|
|
|
|
|
|
|
|
|||||||||||
below |
the |
name, |
age, |
relationship, |
and |
address |
of: |
|
|
|
|
|
|
(Check |
appropriate |
|
p/aces |
below) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
a) |
Wrdow |
or |
Widower, |
|
|
cl |
None |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
cl |
Death |
|
|
Give |
Date |
|
|
|
|
|
|
||||
|
If |
none, |
was Insured |
ever |
married? |
0 |
Yes |
0 |
No |
|
|
If |
yes, |
did |
marriage |
|
terminate |
|
by |
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
0 |
Divorce |
|
|
Give |
Date |
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
b) |
If |
there |
is |
no |
survivrng |
wrdow |
or widower, |
|
list |
all the |
children |
|
|
of |
the |
deceased. |
|
Include |
|
any |
adopted |
child |
or |
illegitimate |
|
child |
stating |
whrch |
class |
it |
|
|
|||||||||
|
IS |
and |
list |
the |
descendants |
|
of |
any |
deceased |
|
child |
or children. |
|
If |
none, |
check |
here |
cl |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
c) |
If |
there |
are |
no |
children |
or |
descendants |
|
of |
chrldren, |
lrst |
the |
survivrng |
|
parent |
or |
parents. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
Is |
father |
deceased? |
0 |
|
Yes |
|
0 |
No |
|
|
|
|
Is |
mother |
|
deceased? |
|
0 |
|
Yes |
|
0 |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
d) |
If |
there |
are |
no |
survivors |
within |
the |
degrees |
Indicated |
in |
(a) |
through |
|
(c). list |
below |
the |
next |
of |
km who may |
|
be |
capable |
|
of |
inheriting |
from |
the deceased |
(brothers, |
sisfers, |
||||||||||||
descendants of deceased brothers, sisters, etc.).
15A NAME |
1 158. AGE 1 |
15C. RELATIONSHIP |
TO DECEASED |
1 |
15D. ADDRESS |
VOTE - Complete Items 16 and 77 ONLY if any of the persons listed above are under age 21.
5 |
NAME |
AND |
ADDRESS |
|
OF GUARDIAN |
FOR ANY MINOR |
CHILDREN |
LISTED |
|
ABOVE IF ONE HAS |
BEEN APPOINTED |
BY THE |
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
COURT (Attach copy or appOmme”f paper issued by court, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
PART |
Ill |
- |
INFORMATION |
CONCERNING |
|
THE |
ESTATE |
OF |
THE |
DECEASED |
|
|
|
|
|
|
|
||||||||
3 |
NAME |
AND |
ADDRESS |
|
OF EXECUTOR |
OR ADMINISTRATOR, |
|
IF ANY. |
APPOINTED |
|
BY THE |
COURT |
TO SETTLE |
|
THE |
ESTATE |
OF |
19 |
IF AN |
EXECUTOR |
OR ADMINISTRATOR |
|
HAS |
NOT BEEN |
||||||||||||
|
THEDECEASED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPOINTED. |
WILL |
ONE |
BE APPOINTED? |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 YES q N0 |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART |
IV |
- |
CERTIFICATION |
BY |
|
CLAIMANT |
|
|
|
|
|
|
|
|
|
|
||||
|
HEREBY |
CERTIFY |
that |
all |
statements |
made |
In |
thus |
claim |
|
are |
true |
to |
the |
best |
of |
my knowledge, |
informatron, |
and |
belief, |
and |
that |
no evidence |
necessary |
to a settlement |
|||||||||||
)f |
this clarm |
is suppressed |
|
or |
wrthheld. |
In |
the |
event |
the |
Insured |
has |
|
not |
previously |
elected |
monthly |
|
Installments. |
I |
request |
that the |
death |
benefit |
be |
paid |
In: |
|
|||||||||
Check |
one) |
|
El |
One |
Sum |
|
|
|
|
III |
36 |
Eaual |
Monthlv |
Installments. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
WARNING |
- |
Any |
rntentronal |
|
false |
statement |
|
in |
thus |
claim |
|
or willful |
misrepresentation |
relative |
thereto |
is |
subject |
to |
punrshment |
by |
a fine |
of not |
more |
than |
$10,000 |
or |
||||||||||
mprisonment |
of not more |
than |
5 |
years, or |
both. |
(16 |
U.S.C. |
1001). |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
IF ADDITIONAL
EXISTING STOCKS OF SGLV 8283, JAN 1991, WILL BE USED.
SPACE IS REQUIRED, ATTACH SEPARATE SIGNED SHEETS.
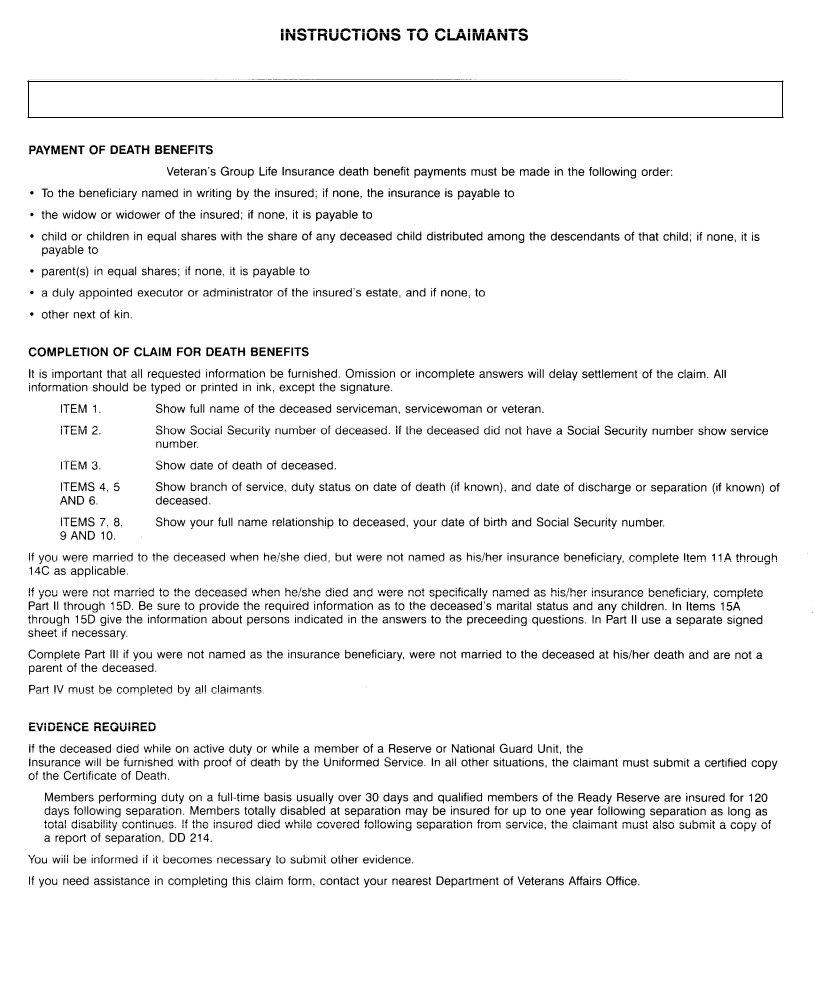
INSTRUCTIONS TO CLAIMANTS
THIS FORM SHOULD BE USED WHEN THE DECEASED HAD INSURANCE IN FORCE UNDER SERVICEMEN’S GROUP LIFE INSURANCE (SGLI) OR VETERANS’ GROUP LIFE INSURANCE (VGLI).
PAYMENT OF DEATH BENEFITS
Under Servicemen’s and Veteran’s Group Life Insurance death benefit payments must be made in the following order:
To the beneficiary named in writing by the insured; if none, the insurance is payable to
the widow or widower of the insured; if none, it is payable to
child or children in equal shares with the share of any deceased child distributed among the descendants of that child; if none, it is payable to
parent(s) in equal shares; if none, it is payable to
a duly appointed executor or administrator of the insured’s estate, and if none, to
other next of kin.
COMPLETION OF CLAIM FOR DEATH BENEFITS
It is important that all requested information be furnished. Omission or incomplete answers will delay settlement of the claim. All information should be typed or printed in ink, except the signature.
ITEM 1. Show full name of the deceased serviceman, servicewoman or veteran.
ITEM 2. Show Social Security number of deceased. If the deceased did not have a Social Security number show service number.
ITEM 3. |
|
Show |
date |
of |
death |
of deceased. |
|
|
|
|
|
|
|
|
|
|
||
ITEMS |
4, |
5 |
Show |
branch |
of service, |
duty status |
on date |
of death |
(if |
known), |
and |
date |
of discharge |
or separation |
(if known) of |
|||
AND 6. |
|
|
deceased. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ITEMS |
7, |
8, |
Show |
your |
full name |
relationship |
to |
deceased, |
your |
date |
of birth |
and |
Social |
Security |
number. |
|
||
9 AND |
10. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If you were married to the deceased |
|
when |
he/she |
died, |
but |
were not |
named |
as |
his/her |
insurance |
beneficiary, |
complete Item |
11A through |
|||||
14C as applicable. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
If you were not married to the deceased when he/she died and were not specifically named as his/her insurance beneficiary, complete Part II through 15D. Be sure to provide the required information as to the deceased’s marital status and any children. In Items 15A through 15D give the information about persons indicated in the answers to the preceeding questions. In Part II use a separate signed sheet if necessary.
Complete Part Ill if you were not named as the insurance beneficiary, were not married to the deceased at his/her death and are not a parent of the deceased.
Part IV must be completed by all claimants
EVIDENCE REQUIRED
If the deceased died while on active duty or while a member of a Reserve or National Guard Unit, the Office of Servicemen’s Group Life Insurance will be furnished with proof of death by the Uniformed Service. In all other situations, the claimant must submit a certified copy of the Certificate of Death.
Members performing duty on a
You will be informed if it becomes necessary to submit other evidence.
If you need assistance in completing this claim form, contact your nearest Department of Veterans Affairs Office.
*lJS Government PrlntlngOftce 1991