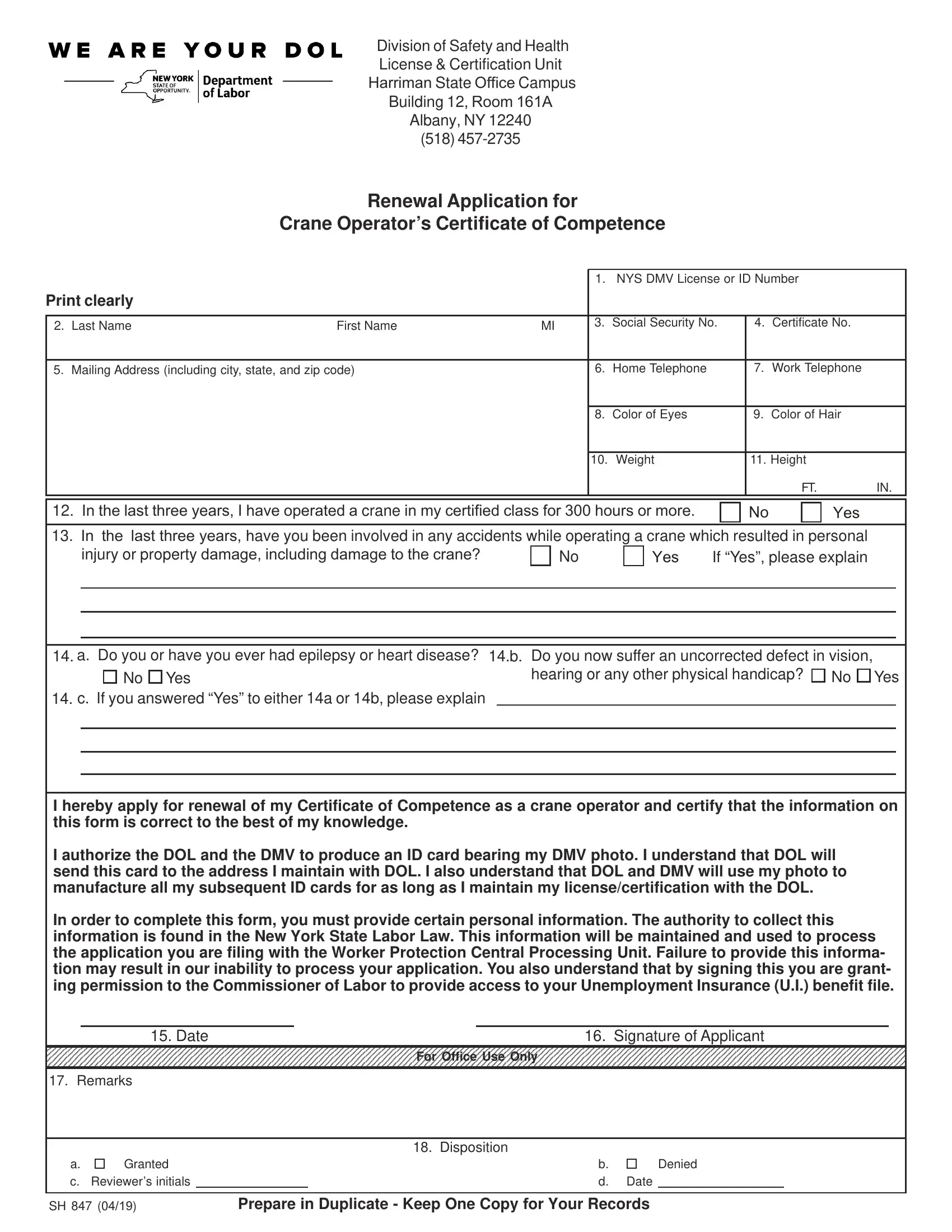
Operating a crane in New York State is a responsibility that requires a recognized level of competence. The Renewal Application for Crane Operator’s Certificate of Competence, known as the SH-847 form, is a key document managed by the New York State Department of Labor Division of Safety and Health License & Certification Unit. This form is essential for crane operators seeking to renew their Certificate of Competence, ensuring they continue to meet the required standards for operating cranes safely. It asks for detailed personal information, including New York State DMV License or ID Number, contact information, physical characteristics, and crane operating experience. Furthermore, it delves into safety concerns by inquiring about any accidents or health conditions that might affect the applicant’s ability to operate a crane. By filling out this form, an applicant not only renews their certification but also affirms their commitment to maintaining a safe operating environment. This process underscores the importance of accountability and safety in crane operations, reflecting the New York State Labor Law's emphasis on protecting workers and the public. The SH-847 form serves as a critical step in this ongoing commitment to safety, where the accurate completion and honest disclosure of the required information play a pivotal role in the certification process.
| Question | Answer |
|---|---|
| Form Name | Sh 847 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | new york state crane operator certificate of competence, nys crane operator license renewal, New_York, 161A |
New York State Department of Labor
Division of Safety and Health
License & Certification Unit Room 161A
State Campus Building 12
Albany NY 12240
(518)
Renewal Application For
Crane Operator’s Certificate of Competence
1. NYS DMV License or ID Number
Print clearly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Last Name |
First Name |
MI |
3. |
Social Security No. |
4. |
Certificate No. |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
5. Mailing Address (including city, state, and zip code) |
|
6. |
Home Telephone |
7. |
Work Telephone |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
8. |
Color of Eyes |
9. |
Color of Hair |
|
|
|
|
|
|
|
|
|
|
|
|
10. |
Weight |
11. Height |
|
|
|
|
|
|
|
|
FT. |
IN. |
12.How many months of crane operating experience have you had since your last application?
13.Have you been involved in any accidents while operating a crane which resulted in personal injury or property
damage, including damage to the crane? |
No |
Yes If “Yes” please explain |
|
|
|
|
|
|
|
|
|
|
|
|
|
14. a. Do you or have you ever had epilepsy or heart disease? 14.b. Do you now suffer an uncorrected defect in vision,
No Yes |
hearing or any other physical handicap? |
No Yes |
14. c. If you answered “Yes” to either 14a or 14b, please explain
I hereby apply for renewal of my Certificate of Competence as a crane operator and certify that the information on this form is correct to the best of my knowledge.
I authorize the DOL and the DMV to produce an ID card bearing my DMV photo. I understand that DOL will send this card to the address I maintain with DOL. I also understand that DOL and DMV will use my photo to manufacture all my subsequent ID cards for as long as I maintain my license/certification with the DOL.
In order to complete this form, you must provide certain personal information. The authority to collect this information is found in the New York State Labor Law. This information will be maintained and used to process the application you are filing with the Worker Protection Central Processing Unit. Failure to provide this informa- tion may result in our inability to process your application. You also understand that by signing this you are grant- ing permission to the Commissioner of Labor to provide access to your Unemployment Insurance (U.I.) benefit file.
15. Date |
16. Signature of Applicant |
For Office Use Only
17. Remarks
|
|
|
18. Disposition |
|
|
|
a. |
Granted |
|
b. |
|
Denied |
|
c. |
Reviewer’s initials |
|
d. |
Date |
||
|
|
|
|
|
|
|
Prepare in Duplicate - Keep One Copy For Your Records |
||||||