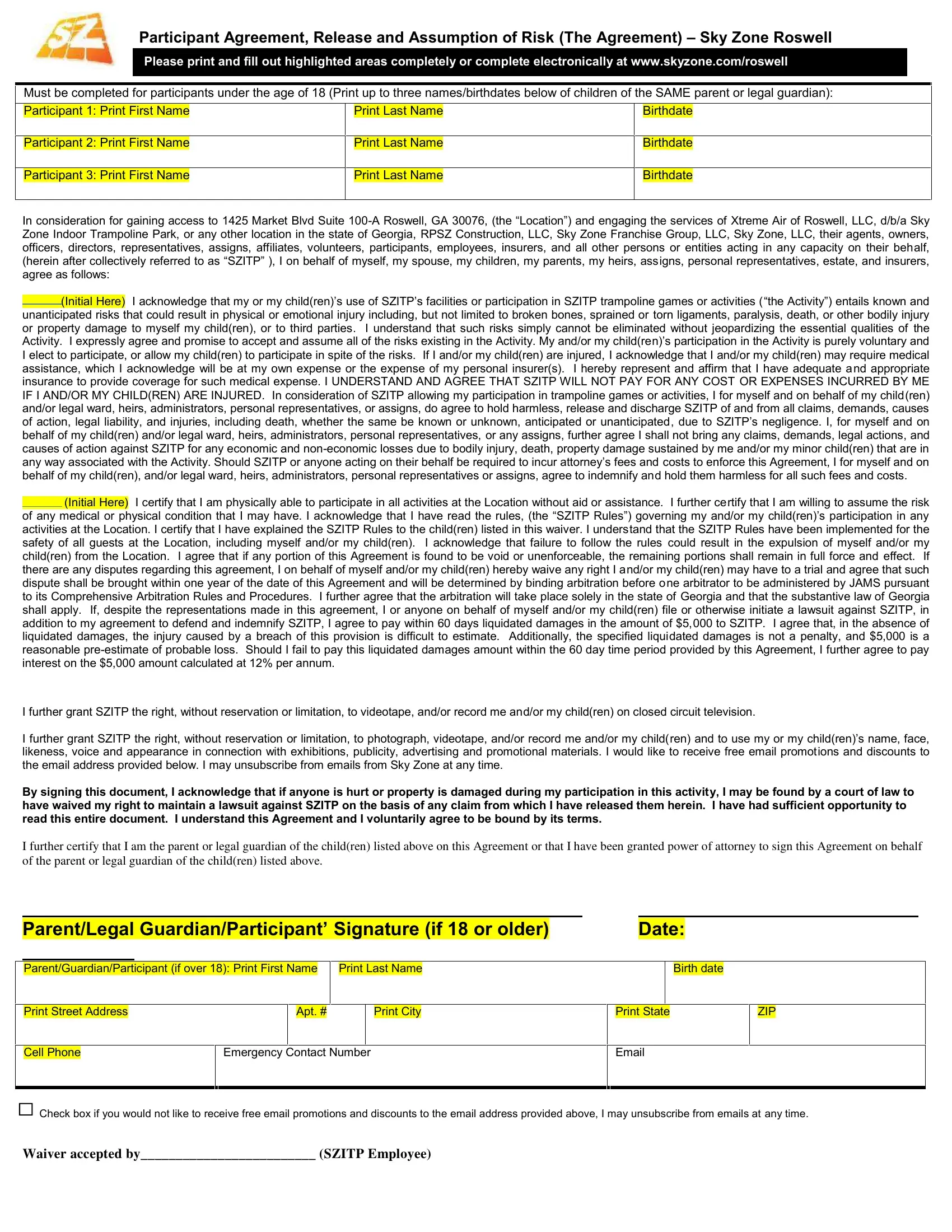
Ensuring the safety and enjoyment of all visitors, Sky Zone Roswell requires participants and their guardians to complete a comprehensive Participant Agreement, Release, and Assumption of Risk form. This document is a crucial step for anyone looking to engage in the exciting activities offered at 1425 Market Blvd Suite 100-A, Roswell, GA 30076, operated by Xtreme Air of Roswell, LLC, amongst other related entities. The form is designed to be filled out by adults for up to three children under the age of 18, sharing the same parent or legal guardian, detailing the participants' names and birthdates. By acknowledging the inherent risks involved in participating in trampoline games or activities, signatories agree to assume all risks and agree not to hold Sky Zone responsible for any injuries or damages that might occur. This agreement stipulates that any medical expenses incurred due to injuries at the facility will not be covered by Sky Zone, emphasizing the importance of having personal insurance. Additionally, the document includes provisions regarding the enforcement of the agreement, including arbitration in Georgia and specific clauses concerning the use of photographic and video material of participants. The agreement also outlines the expectations of participants regarding the observance of Sky Zone rules for safety and the legal implications of consenting to this document. This introductory guide to the agreement highlights the comprehensive measures Sky Zone Roswell employs to ensure a safe and enjoyable environment for all guests while clarifying the legal responsibilities assumed by participants and their guardians.
| Question | Answer |
|---|---|
| Form Name | Sky Zone Roswell Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | LLC, sky zone roswell waiver, SZITP, roswell agreement |
Participant Agreement, Release and Assumption of Risk (The Agreement) Sky Zone Roswell
Please print and fill out highlighted areas completely or complete electronically at www.skyzone.com/roswell
Must be completed for participants under the age of 18 (Print up to three names/birthdates below of children of the SAME parent or legal guardian):
|
Participant 1: Print First Name |
|
|
Print Last Name |
|
|
Birthdate |
|
|
|
|
|
|
|
|
|
|
Participant 2: Print First Name
Print Last Name
Birthdate
Participant 3: Print First Name
Print Last Name
Birthdate
In consideration for gaining access to 1425 Market Blvd Suite
(Initial Here) I acknowledge that my or my child(ren) s use of SZITP s facilities or participation in SZITP trampoline games or activities ( the Activity ) entails known and unanticipated risks that could result in physical or emotional injury including, but not limited to broken bones, sprained or torn ligaments, paralysis, death, or other bodily injury or property damage to myself my child(ren), or to third parties. I understand that such risks simply cannot be eliminated without jeopardizing the essential qualities of the Activity. I expressly agree and promise to accept and assume all of the risks existing in the Activity. My and/or my child(ren) s participation in the Activity is purely voluntary and I elect to participate, or allow my child(ren) to participate in spite of the risks. If I and/or my child(ren) are injured, I acknowledge that I and/or my child(ren) may require medical assistance, which I acknowledge will be at my own expense or the expense of my personal insurer(s). I hereby represent and affirm that I have adequate and appropriate insurance to provide coverage for such medical expense. I UNDERSTAND AND AGREE THAT SZITP WILL NOT PAY FOR ANY COST OR EXPENSES INCURRED BY ME IF I AND/OR MY CHILD(REN) ARE INJURED. In consideration of SZITP allowing my participation in trampoline games or activities, I for myself and on behalf of my child(ren) and/or legal ward, heirs, administrators, personal representatives, or assigns, do agree to hold harmless, release and discharge SZITP of and from all claims, demands, causes of action, legal liability, and injuries, including death, whether the same be known or unknown, anticipated or unanticipated, due to SZITP s negligence. I, for myself and on behalf of my child(ren) and/or legal ward, heirs, administrators, personal representatives, or any assigns, further agree I shall not bring any claims, demands, legal actions, and causes of action against SZITP for any economic and
(Initial Here) I certify that I am physically able to participate in all activities at the Location without aid or assistance. I further certify that I am willing to assume the risk of any medical or physical condition that I may have. I acknowledge that I have read the rules, (the SZITP Rules ) governing my and/or my child(ren) s participation in any activities at the Location. I certify that I have explained the SZITP Rules to the child(ren) listed in this waiver. I understand that the SZITP Rules have been implemented for the safety of all guests at the Location, including myself and/or my child(ren). I acknowledge that failure to follow the rules could result in the expulsion of myself and/or my child(ren) from the Location. I agree that if any portion of this Agreement is found to be void or unenforceable, the remaining portions shall remain in full force and effect. If there are any disputes regarding this agreement, I on behalf of myself and/or my child(ren) hereby waive any right I and/or my child(ren) may have to a trial and agree that such dispute shall be brought within one year of the date of this Agreement and will be determined by binding arbitration before one arbitrator to be administered by JAMS pursuant to its Comprehensive Arbitration Rules and Procedures. I further agree that the arbitration will take place solely in the state of Georgia and that the substantive law of Georgia shall apply. If, despite the representations made in this agreement, I or anyone on behalf of myself and/or my child(ren) file or otherwise initiate a lawsuit against SZITP, in addition to my agreement to defend and indemnify SZITP, I agree to pay within 60 days liquidated damages in the amount of $5,000 to SZITP. I agree that, in the absence of liquidated damages, the injury caused by a breach of this provision is difficult to estimate. Additionally, the specified liquidated damages is not a penalty, and $5,000 is a reasonable
I further grant SZITP the right, without reservation or limitation, to videotape, and/or record me and/or my child(ren) on closed circuit television.
I further grant SZITP the right, without reservation or limitation, to photograph, videotape, and/or record me and/or my child(ren) and to use my or my child(ren) s name, face, likeness, voice and appearance in connection with exhibitions, publicity, advertising and promotional materials. I would like to receive free email promotions and discounts to the email address provided below. I may unsubscribe from emails from Sky Zone at any time.
By signing this document, I acknowledge that if anyone is hurt or property is damaged during my participation in this activity, I may be found by a court of law to have waived my right to maintain a lawsuit against SZITP on the basis of any claim from which I have released them herein. I have had sufficient opportunity to read this entire document. I understand this Agreement and I voluntarily agree to be bound by its terms.
I further certify that I am the parent or legal guardian of the child(ren) listed above on this Agreement or that I have been granted power of attorney to sign this Agreement on behalf of the parent or legal guardian of the child(ren) listed above.
Parent/Legal Guardian/Participant Signature (if 18 or older) |
|
|
Date: |
|
Parent/Guardian/Participant (if over 18): Print First Name
Print Last Name
Birth date
Print Street Address
Apt. #
Print City
Print State
ZIP
Cell Phone
Emergency Contact Number
Check box if you would not like to receive free email promotions and discounts to the email address provided above, I may unsubscribe from emails at any time.
Waiver accepted by_________________________ (SZITP Employee)