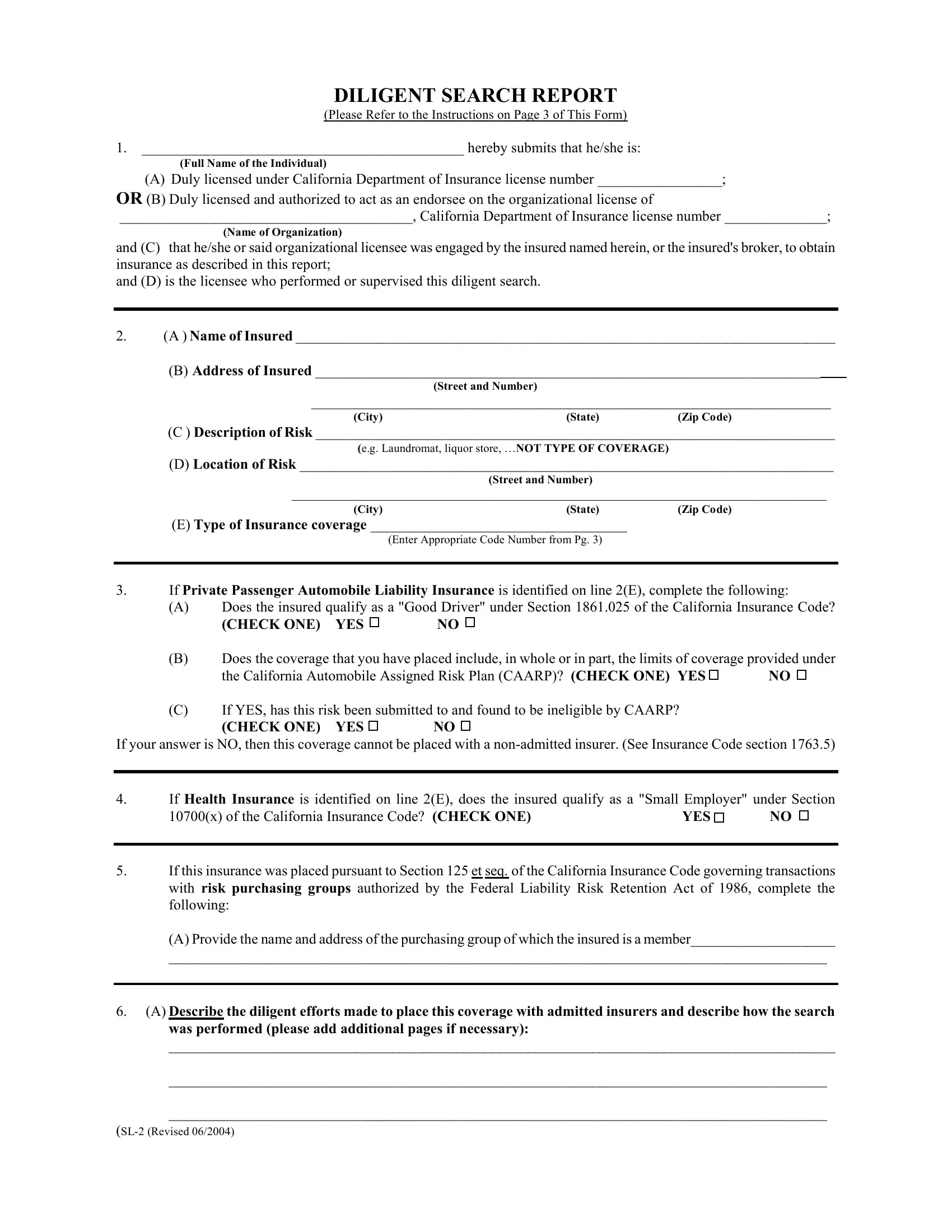
DILIGENT SEARCH REPORT
(Please Refer to the Instructions on Page 3 of This Form)
1.____________________________________________ hereby submits that he/she is:
(Full Name of the Individual)
(A) Duly licensed under California Department of Insurance license number _________________;
OR (B) Duly licensed and authorized to act as an endorsee on the organizational license of
________________________________________, California Department of Insurance license number ______________;
(Name of Organization)
and (C) that he/she or said organizational licensee was engaged by the insured named herein, or the insured's broker, to obtain insurance as described in this report;
and (D) is the licensee who performed or supervised this diligent search.
2.(A ) Name of Insured __________________________________________________________________________
(B) Address of Insured _____________________________________________________________________
(Street and Number)
_______________________________________________________________________
(City)(State) (Zip Code)
(C ) Description of Risk _______________________________________________________________________
(e.g. Laundromat, liquor store, …NOT TYPE OF COVERAGE)
(D) Location of Risk _________________________________________________________________________
(Street and Number)
_________________________________________________________________________________
(City)(State) (Zip Code)
(E) Type of Insurance coverage ___________________________________
(Enter Appropriate Code Number from Pg. 3)
3.If Private Passenger Automobile Liability Insurance is identified on line 2(E), complete the following:
(A)Does the insured qualify as a "Good Driver" under Section 1861.025 of the California Insurance Code?
(B)Does the coverage that you have placed include, in whole or in part, the limits of coverage provided under
the California Automobile Assigned Risk Plan (CAARP)? (CHECK ONE) YES |
NO |
(C)If YES, has this risk been submitted to and found to be ineligible by CAARP?
If your answer is NO, then this coverage cannot be placed with a non-admitted insurer. (See Insurance Code section 1763.5)
4.If Health Insurance is identified on line 2(E), does the insured qualify as a "Small Employer" under Section
10700(x) of the California Insurance Code? (CHECK ONE) |
YES |
NO |
|
|
|
5.If this insurance was placed pursuant to Section 125 et seq. of the California Insurance Code governing transactions with risk purchasing groups authorized by the Federal Liability Risk Retention Act of 1986, complete the following:
(A) Provide the name and address of the purchasing group of which the insured is a member____________________
__________________________________________________________________________________________
6.(A) Describe the diligent efforts made to place this coverage with admitted insurers and describe how the search was performed (please add additional pages if necessary):
_____________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
(SL-2 (Revised 06/2004)
(B) If search was performed by someone other than the person named on line 1, please provide full name of that individual:
___________________________________________________
7.(A) Was the risk described in Section 2 submitted by you or by someone under your supervision to at least (3)
insurers that are admitted in California and who actually write the type of insurance described on lines 2(C) and
(B) If YES, please complete ALL sections of the following table; if NO, skip to Section 8:
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full Name of Admitted Company |
First & Last Name of Company |
Check if |
Month, |
Year |
|
Declination |
|
|
Representative AND Telephone |
Employee (E) |
of Declination |
|
Code* |
|
|
Number |
|
|
or Agent (A) |
|
|
|
|
|
1. |
|
______________________________ |
|
E ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
- |
|
|
A ( |
) |
/ |
|
|
|
|
|
|
or “Online Declination” |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Website________________________ |
|
|
|
|
|
|
|
|
2. |
|
|
|
|
|
|
E ( |
) |
|
|
|
|
|
|
|
______________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
- |
|
|
A ( |
) |
/ |
|
|
|
|
|
|
or “Online Declination” |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Website________________________ |
|
|
|
|
|
|
|
|
3. |
|
_______________________________ |
|
E ( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
- |
|
|
A ( |
) |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or “Online Declination” |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Website________________________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
*Declination Codes: 1 - Company's capacity reached |
2-underwriting reason |
3-refused to state |
4-other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8.If 7(A) was answered NO, complete the following:
(A) Did you determine that fewer than 3 admitted insurers actually write the type of insurance described on lines
2(C) and 2(E)? (CHECK ONE) YES |
NO |
(B)If NO, please explain in detail why the risk was submitted to less than three admitted insurers in California that write this type of insurance.
_______________________________________________________________________________________
___________________________________________________________________________________________
________________________________________________________________________________________
(C) If YES, please describe how you made this determination.________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
The undersigned licensee hereby certifies that this report is true and correct, and that this risk is not being placed with a non- admitted insurer for the sole purpose of securing a rate or premium lower than the lowest rate or premium available from an admitted insurer.
___________________________________________________________________ |
__________________ |
(Signature of Licensee Named on Line 1) |
(Date) |
INSTRUCTIONS
SECTION 1: Please provide the full name of the licensed individual who performed or supervised the diligent search. If the search was performed under the individual’s license number, enter his/her license number in section (A) or if the individual was authorized as an endorsee under an organizational license, enter the name of the organization and its license number in section (B).
SECTION 6: Please provide a complete response on section (A). Note: The Insurance Commissioner or his designee may require the surplus line broker to conduct a further or additional search among admitted insurers for similar placements in the future. [California Insurance Code Section 1763(b)] An incomplete response may unnecessarily result in a request for a further search to be conducted. If the individual named on line 1 did not perform the diligent search, please provide the full name of the individual who performed the search on section (B).
SECTION 7(B): To avoid mis-identification among insurers with similar names, please provide the complete name of the admitted insurer as listed in the CDI Official Publication of Admitted Companies.
Insurer group names, such as Cigna Group, Chubb Group, California Ins. Group, Hartford Group, etc., are acceptable if the person performing the search verifies that the representative of the group, who declines the risk, does in fact represent an admitted insurer in the group that actually writes the particular type of insurance being sought.
IMPORTANT: Persons who are licensed only as an agent may only submit a risk to admitted insurers that have appointed them as their agent. Agents are not authorized to offer a risk to admitted insurers for which they are not appointed agents. A search which is limited to only those companies that have appointed the agent may not necessarily constitute a diligent search of the admitted market.
WHAT TO FILE: This report must be filed as an attachment to the Report of Placement. (CDI Form SL-1).
WHERE TO FILE: The SL-1 and this report are to be filed by the surplus line broker with The Surplus Line Association of California within 60 days of placement of coverage with non-admitted insurer(s).
MULTIPLE LICENSEES CONDUCTING SEARCH: If two or more licensees conduct a diligent search of admitted insurers, then each licensee must complete a diligent search report (CDI Form SL-2). All such reports should be attached to the SL-1.
CODE TYPE OF INSURANCE |
CODE TYPE OF INSURANCE |
050 |
Auto Liability-Private |
510 |
Aviation |
051 |
Auto Liability-Commercial |
550 |
Errors & Omissions-All Others |
100 |
Auto Physical Damage-Private |
551 |
Errors & Omission-Directors & Officers |
101 |
Auto Physical Damage-Commercial |
600 |
Malpractice-All Other |
150 |
Crime |
606 |
Malpractice-Hospitals |
151 |
Crime-Kidnap & Ransom |
650 |
Miscellaneous |
200 |
Combined Auto Liability & P.D.-Private |
651 |
Miscellaneous-Glass |
201 |
Combined Auto Liability & P.D.-Comm. |
652 |
Miscellaneous-Boiler & Machinery |
300 |
Excess Liability (Incl. Umbrella) |
653 |
Miscellaneous-Nuclear Risks |
350 |
Fidelity Surety & Bonds-Bonds |
655 |
Miscellaneous-Political Risks |
351 |
Fidelity Surety & Bonds-Fidelity |
700 |
Accident |
400 |
Fire-Single Family Dwelling, Duplex |
701 |
Accident-Disability Income |
401 |
Fire-Commercial |
702 |
Accident-Group Health Ins. |
402 |
Fire-Homeowners |
703 |
Accident-Ind. Health Ins. |
403 |
Fire-Homeowners Multiple Peril |
800 |
Garage Liability |
404 |
Fire-Farm Owners Multiple Peril |
980 |
Excess Workers Compensation |
414 |
Residential Earthquake |
990 |
Commercial Property-All Risk |
450 |
Inland Marine |
994 |
Commercial Property-Special Multi-Peril |
500 |
General Liability |
996 |
Commercial Property-DIC |
501 |
Gen. Liability-Pollution Legal Liability |
997 |
Commercial Property-Earthquake |
502 |
General Liability-Product Tampering |
998 |
Commercial Property-Terrorism |
|
|
999 |
CommercialProperty-Special Multi-Perilw/Terrorism |
(This list does not include those coverages on the export list. An updated export coverage list is published every year by the California Dept. of Insurance.)