
ssa 789 u4 form printable can be completed online without difficulty. Just try FormsPal PDF editing tool to accomplish the job without delay. Our editor is constantly evolving to provide the very best user experience achievable, and that is because of our dedication to continual development and listening closely to feedback from customers. Here's what you'd have to do to start:
Step 1: Access the form inside our tool by hitting the "Get Form Button" above on this webpage.
Step 2: The tool allows you to customize PDF files in various ways. Improve it with personalized text, correct what's originally in the file, and place in a signature - all readily available!
Be mindful while completing this pdf. Make sure that each field is filled in accurately.
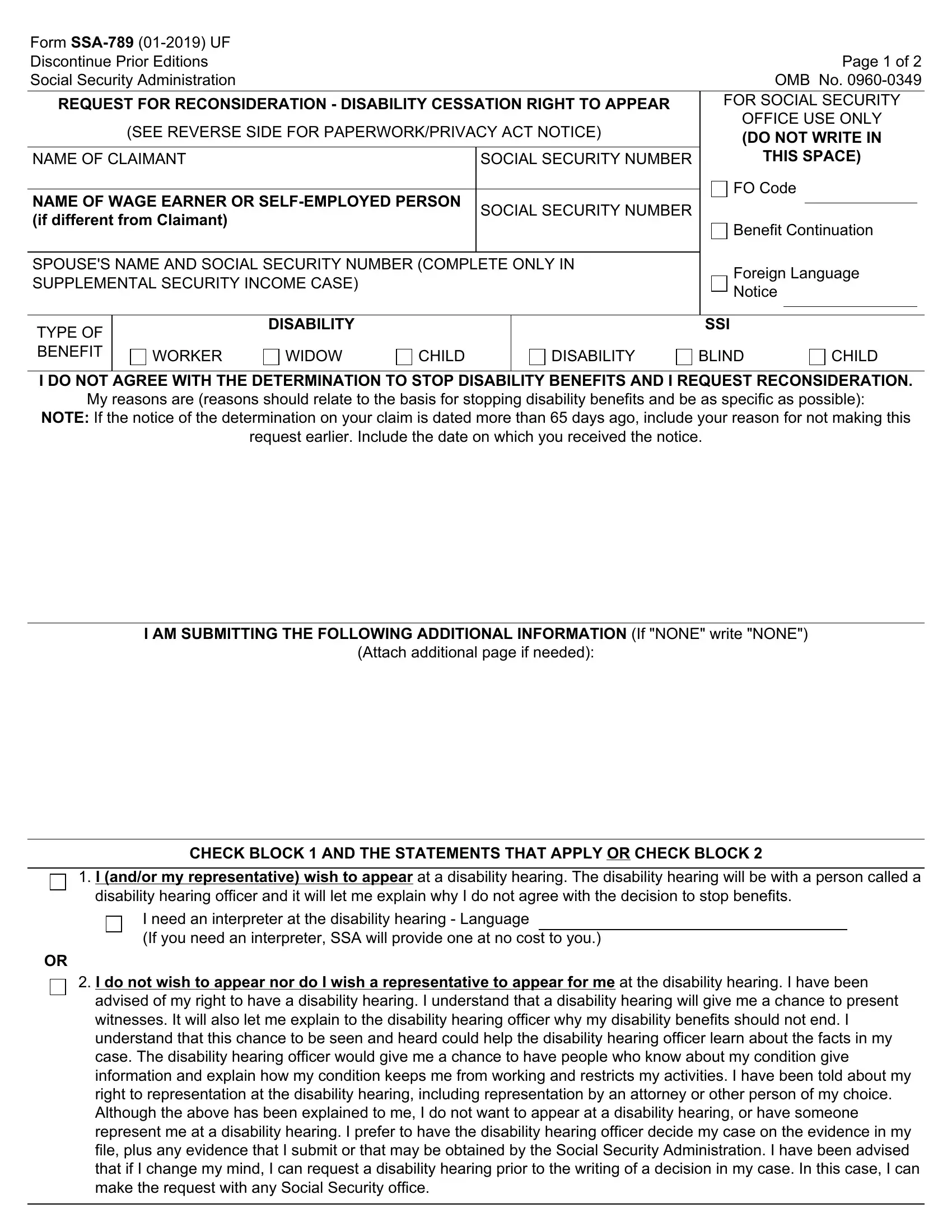
1. It's important to complete the ssa 789 u4 form printable properly, hence be mindful while working with the segments including these specific blanks:
2. After the last segment is completed, you're ready insert the necessary particulars in Attach additional page if needed, CHECK BLOCK AND THE STATEMENTS, I andor my representative wish to, disability hearing officer and it, I need an interpreter at the, I do not wish to appear nor do I, and advised of my right to have a so you can go to the next step.
In terms of I need an interpreter at the and Attach additional page if needed, make sure you do everything correctly in this section. The two of these could be the most significant ones in the file.
3. This third part is quite straightforward, CLAIMANT SIGNATURE, SIGNATURE OR NAME OF CLAIMANTS, STREET ADDRESS, REPRESENTATIVES ADDRESS, CITY, STATE ZIP CODE, CITY, STATE ZIP CODE, TELEPHONE NUMBER, DATE, TELEPHONE NUMBER, DATE, Witnesses are required ONLY if, SIGNATURE OF WITNESS, and SIGNATURE OF WITNESS - these blanks will need to be completed here.
Step 3: Ensure your information is right and simply click "Done" to progress further. Get hold of your ssa 789 u4 form printable as soon as you join for a 7-day free trial. Instantly view the pdf file in your FormsPal account page, together with any modifications and changes conveniently kept! With FormsPal, you can certainly complete forms without being concerned about personal data incidents or records being distributed. Our protected platform helps to ensure that your personal information is maintained safely.