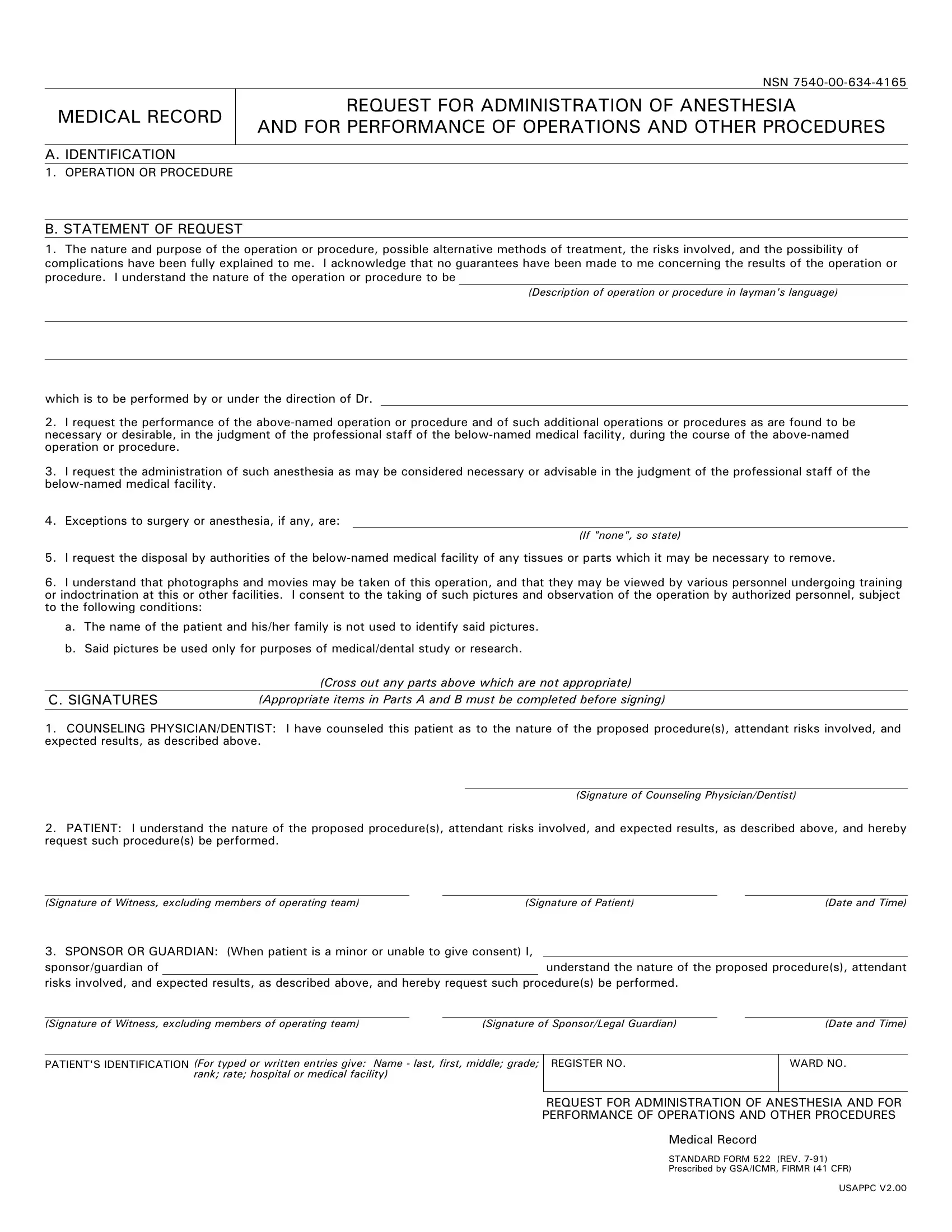
The Standard Form 522, known as the Medical Record Request for Administration of Anesthesia and for Performance of Operations and Other Procedures, serves a critical function within medical and dental facilities, particularly in the context of documenting consent. This comprehensive form encapsulates several key areas: the identification of the operation or procedure in question, a detailed statement of request wherein the patient acknowledges understanding the nature and implications of the procedure, alternatives, risks, and absences of guarantees regarding outcomes. Furthermore, it accommodates the possibility of additional necessary operations discovered during the procedure, details regarding anesthesia, exceptions to surgery or anesthesia if any, and protocols for the disposal of removed tissues or parts. Moreover, the form addresses patient consent for the taking of photographs or movies for medical or dental study or research purposes, ensuring privacy and ethical standards are upheld. The signature section mandates confirmation from the counseling physician or dentist, the patient, or the sponsor/guardian in cases where the patient is a minor or unable to consent, solidifying the shared understanding and agreement on the procedure and its ancillary aspects. This robust document, prescribed by GSA/ICMR and revised as of July 1991, underscores the paramount importance of informed consent in the medical field, ensuring that all parties involved are adequately informed and agreeable to the proceedings as detailed within the medical or dental facilities' operational framework.
| Question | Answer |
|---|---|
| Form Name | Standard Form 522 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | GSA, FIRMR, standard form 522, 522 |
NSN
MEDICAL RECORD
REQUEST FOR ADMINISTRATION OF ANESTHESIA
AND FOR PERFORMANCE OF OPERATIONS AND OTHER PROCEDURES
A. IDENTIFICATION
1. OPERATION OR PROCEDURE
B. STATEMENT OF REQUEST
1.The nature and purpose of the operation or procedure, possible alternative methods of treatment, the risks involved, and the possibility of complications have been fully explained to me. I acknowledge that no guarantees have been made to me concerning the results of the operation or procedure. I understand the nature of the operation or procedure to be
(Description of operation or procedure in layman's language)
which is to be performed by or under the direction of Dr.
2.I request the performance of the
3.I request the administration of such anesthesia as may be considered necessary or advisable in the judgment of the professional staff of the
4.Exceptions to surgery or anesthesia, if any, are:
(If "none", so state)
5.I request the disposal by authorities of the
6.I understand that photographs and movies may be taken of this operation, and that they may be viewed by various personnel undergoing training or indoctrination at this or other facilities. I consent to the taking of such pictures and observation of the operation by authorized personnel, subject to the following conditions:
a.The name of the patient and his/her family is not used to identify said pictures.
b.Said pictures be used only for purposes of medical/dental study or research.
|
(Cross out any parts above which are not appropriate) |
C. SIGNATURES |
(Appropriate items in Parts A and B must be completed before signing) |
1.COUNSELING PHYSICIAN/DENTIST: I have counseled this patient as to the nature of the proposed procedure(s), attendant risks involved, and expected results, as described above.
(Signature of Counseling Physician/Dentist)
2.PATIENT: I understand the nature of the proposed procedure(s), attendant risks involved, and expected results, as described above, and hereby request such procedure(s) be performed.
(Signature of Witness, excluding members of operating team)(Signature of Patient)(Date and Time)
3. SPONSOR OR GUARDIAN: (When patient is a minor or unable to give consent) I, |
|
sponsor/guardian of |
understand the nature of the proposed procedure(s), attendant |
risks involved, and expected results, as described above, and hereby request such procedure(s) be performed.
(Signature of Witness, excluding members of operating team) |
(Signature of Sponsor/Legal Guardian) |
(Date and Time) |
PATIENT'S IDENTIFICATION (For typed or written entries give: Name - last, first, middle; grade;
rank; rate; hospital or medical facility)
REGISTER NO.
WARD NO.
REQUEST FOR ADMINISTRATION OF ANESTHESIA AND FOR PERFORMANCE OF OPERATIONS AND OTHER PROCEDURES
Medical Record
STANDARD FORM 522 (REV.
Prescribed by GSA/ICMR, FIRMR (41 CFR)
USAPPC V2.00