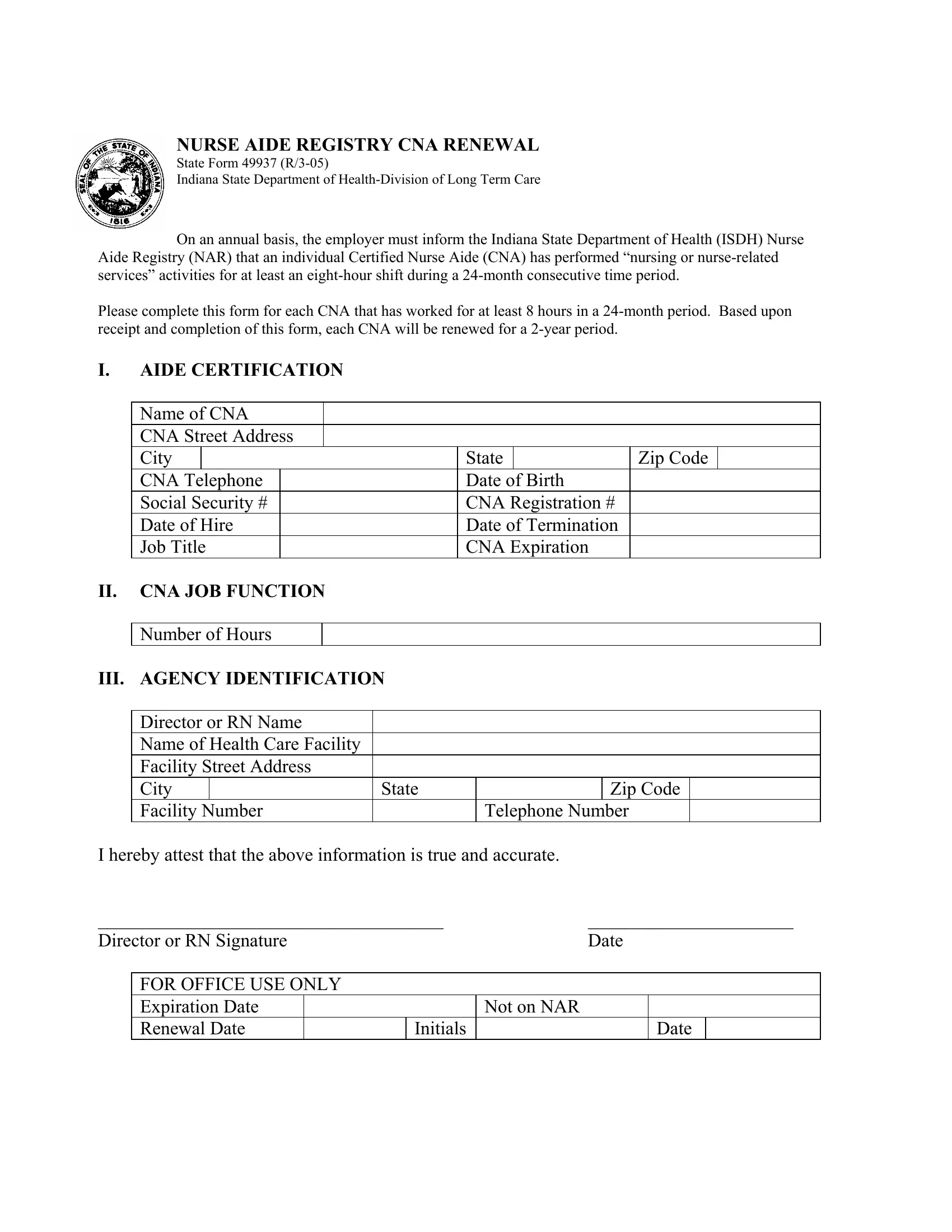
In the realm of healthcare, ensuring that Certified Nurse Aides (CNAs) maintain their credentials is paramount not only for the quality of patient care but also for regulatory compliance. The State 49937 form, designated by the Indiana State Department of Health-Division of Long Term Care, plays a crucial role in this process. This form serves as a renewal application for CNAs to continue their certification with the Nurse Aide Registry (NAR). It requires annual submission by employers to attest that a CNA has actively contributed to nursing or nurse-related services for a minimum of one eight-hour shift within a 24-month consecutive time period. The completion and submission of State Form 49937 ensure that a CNA's registration is renewed for another two-year period. It encompasses various sections including aide certification details, job function information, and agency identification, alongside mandatory attestation by the director or a registered nurse (RN) of the healthcare facility. With accurate and prompt submission, this form guarantees that CNAs remain listed on the Nurse Aide Registry, enabling them to continue their critical work in healthcare settings across Indiana.
| Question | Answer |
|---|---|
| Form Name | State Form 49937 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Expiration, CERTIFICATION, CNA, ISDH |
NURSE AIDE REGISTRY CNA RENEWAL
State Form 49937
Indiana State Department of
On an annual basis, the employer must inform the Indiana State Department of Health (ISDH) Nurse Aide Registry (NAR) that an individual Certified Nurse Aide (CNA) has performed “nursing or
Please complete this form for each CNA that has worked for at least 8 hours in a
I.AIDE CERTIFICATION
Name of CNA
CNA Street Address
City |
|
|
State |
|
Zip Code |
|
CNA Telephone |
|
Date of Birth |
|
|
||
Social Security # |
|
CNA Registration # |
|
|
||
Date of Hire |
|
Date of Termination |
|
|
||
Job Title |
|
CNA Expiration |
|
|
||
II.CNA JOB FUNCTION Number of Hours
III. AGENCY IDENTIFICATION
Director or RN Name |
|
|
Name of Health Care Facility |
|
|
Facility Street Address |
|
|
City |
State |
Zip Code |
Facility Number |
|
Telephone Number |
I hereby attest that the above information is true and accurate.
_____________________________________ |
______________________ |
|||||
Director or RN Signature |
|
Date |
||||
|
|
|
|
|
|
|
|
FOR OFFICE USE ONLY |
|
|
|
|
|
|
Expiration Date |
|
|
Not on NAR |
|
|
|
Renewal Date |
|
Initials |
|
Date |
|