
Dealing with PDF documents online is definitely very simple with this PDF tool. Anyone can fill in tdi 45 form here within minutes. Our tool is consistently evolving to present the best user experience possible, and that's thanks to our dedication to continual enhancement and listening closely to comments from users. Should you be looking to get started, here's what it takes:
Step 1: Hit the "Get Form" button above on this webpage to get into our PDF editor.
Step 2: With our state-of-the-art PDF editor, you'll be able to do more than just fill in blanks. Express yourself and make your forms appear perfect with custom text added, or modify the original content to perfection - all supported by the capability to add stunning graphics and sign it off.
It's an easy task to fill out the pdf using this helpful tutorial! Here is what you have to do:
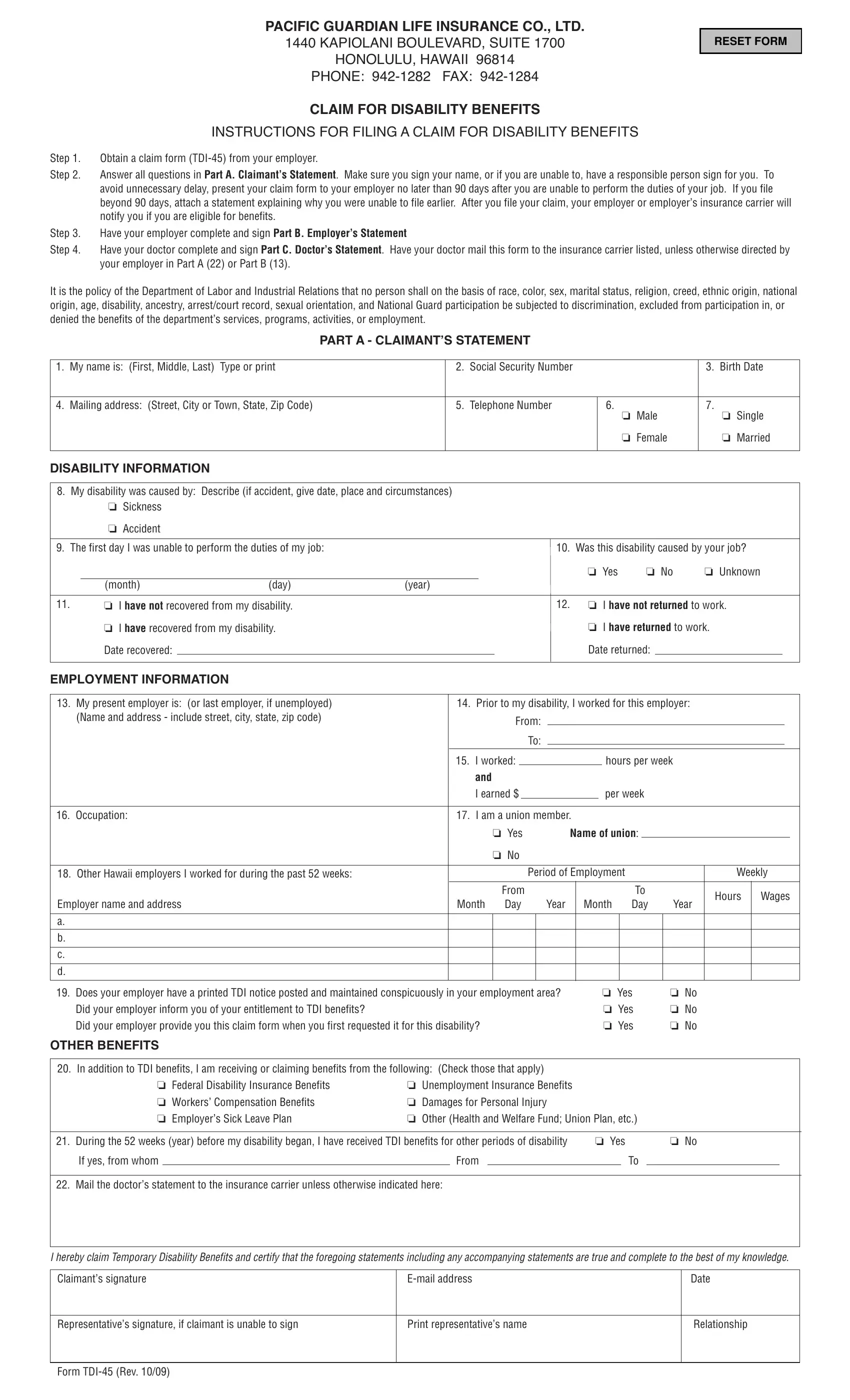
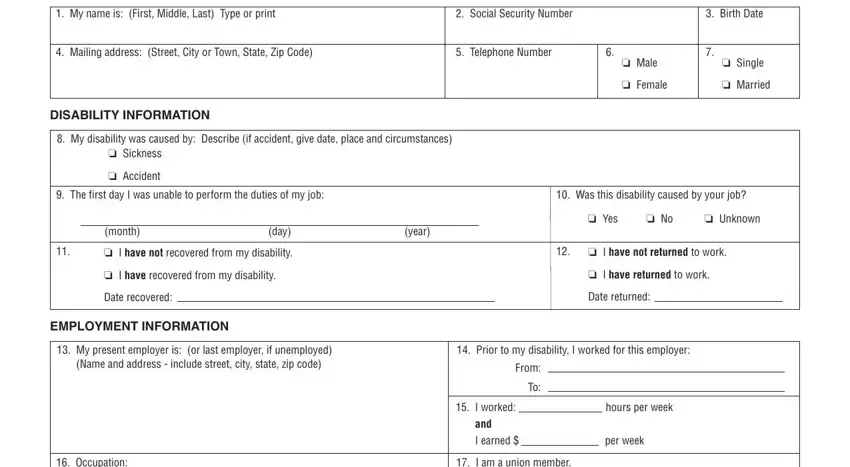
1. When filling out the tdi 45 form, ensure to complete all needed blank fields within the associated form section. It will help speed up the process, making it possible for your details to be processed efficiently and accurately.
2. When this part is done, go on to type in the relevant information in all these - Occupation, Other Hawaii employers I worked, Employer name and address a b c d, I am a union member, o Yes Name of union, o No, From, Hours Wages, Period of Employment, Weekly, Month Day Year, Month Day Year, Does your employer have a printed, Did your employer inform you of, and o No o No o No.
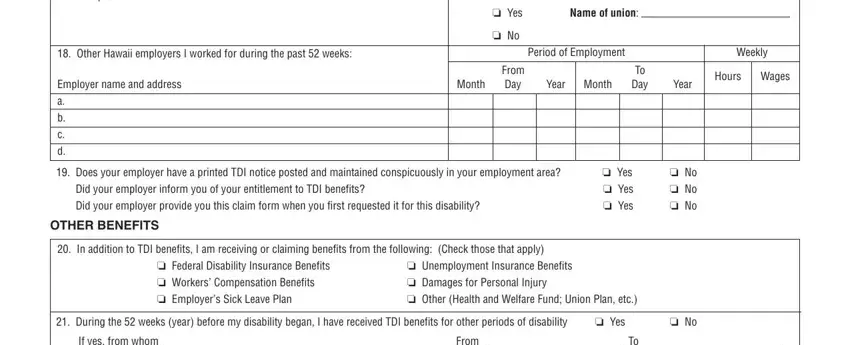
It is easy to make an error when filling out your Did your employer inform you of, thus you'll want to take another look prior to when you finalize the form.
3. In this part, have a look at Mail the doctors statement to the, I hereby claim Temporary, Claimants signature, Email address, Date, Representatives signature if, Print representatives name, Relationship, and Form TDI Rev. Each one of these have to be taken care of with greatest precision.
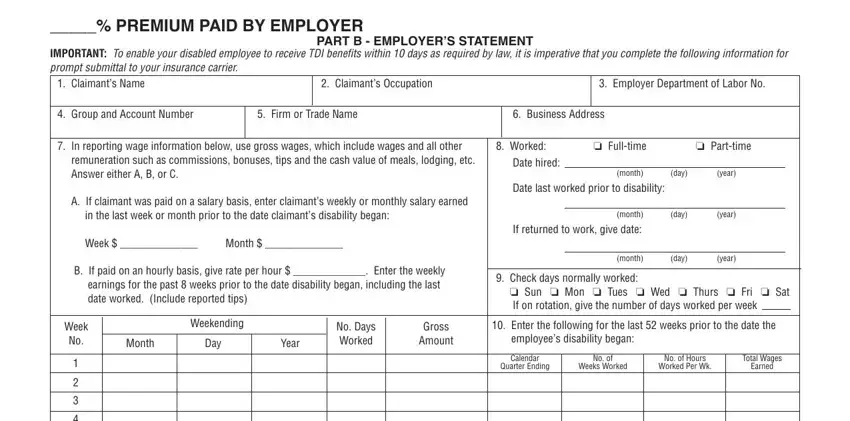
4. This fourth subsection comes next with the next few fields to look at: PREMIUM PAID BY EMPLOYER, PART B EMPLOYERS STATEMENT, IMPORTANT To enable your disabled, Claimants Name, Claimants Occupation, Employer Department of Labor No, Group and Account Number, Firm or Trade Name, Business Address, In reporting wage information, Worked o Fulltime, o Parttime, remuneration such as commissions, Date hired, and month day year.
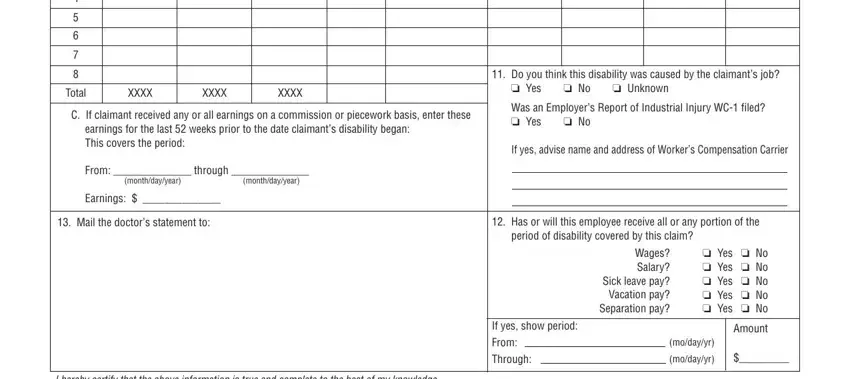
5. Finally, this final section is precisely what you'll have to complete before using the document. The blanks at issue include the following: Total, XXXX, XXXX, XXXX, C If claimant received any or all, earnings for the last weeks prior, From through, monthdayyear, monthdayyear, Earnings, Mail the doctors statement to, Do you think this disability was, o Yes o No o Unknown, Was an Employers Report of, and If yes advise name and address of.
Step 3: Make sure that your details are accurate and then just click "Done" to proceed further. Join FormsPal right now and instantly get tdi 45 form, set for download. All modifications you make are saved , which enables you to edit the document further anytime. With FormsPal, you can complete forms without worrying about personal data leaks or entries getting shared. Our secure system makes sure that your personal information is kept safe.