
Should you would like to fill out annual tb screening questionnaire form, you don't have to download and install any sort of programs - simply try using our online PDF editor. FormsPal development team is relentlessly endeavoring to enhance the editor and help it become much better for people with its many functions. Take full advantage of present-day modern opportunities, and discover a heap of unique experiences! Starting is effortless! All that you should do is stick to the next basic steps down below:
Step 1: Open the PDF form inside our editor by clicking on the "Get Form Button" above on this page.
Step 2: Using our handy PDF tool, you can actually accomplish more than simply complete blank fields. Edit away and make your documents look great with customized textual content added in, or fine-tune the original input to perfection - all that supported by the capability to insert your own images and sign the document off.
This document will need some specific information; in order to guarantee accuracy, please make sure to pay attention to the next recommendations:
1. When filling out the annual tb screening questionnaire form, make sure to complete all needed fields in its corresponding area. It will help to facilitate the process, enabling your information to be processed without delay and appropriately.
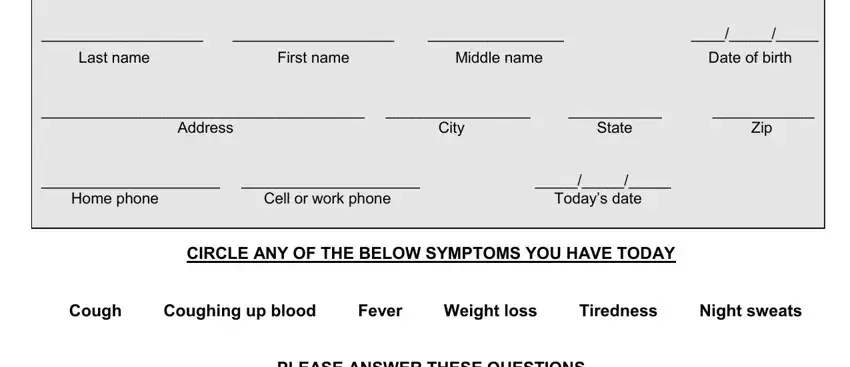
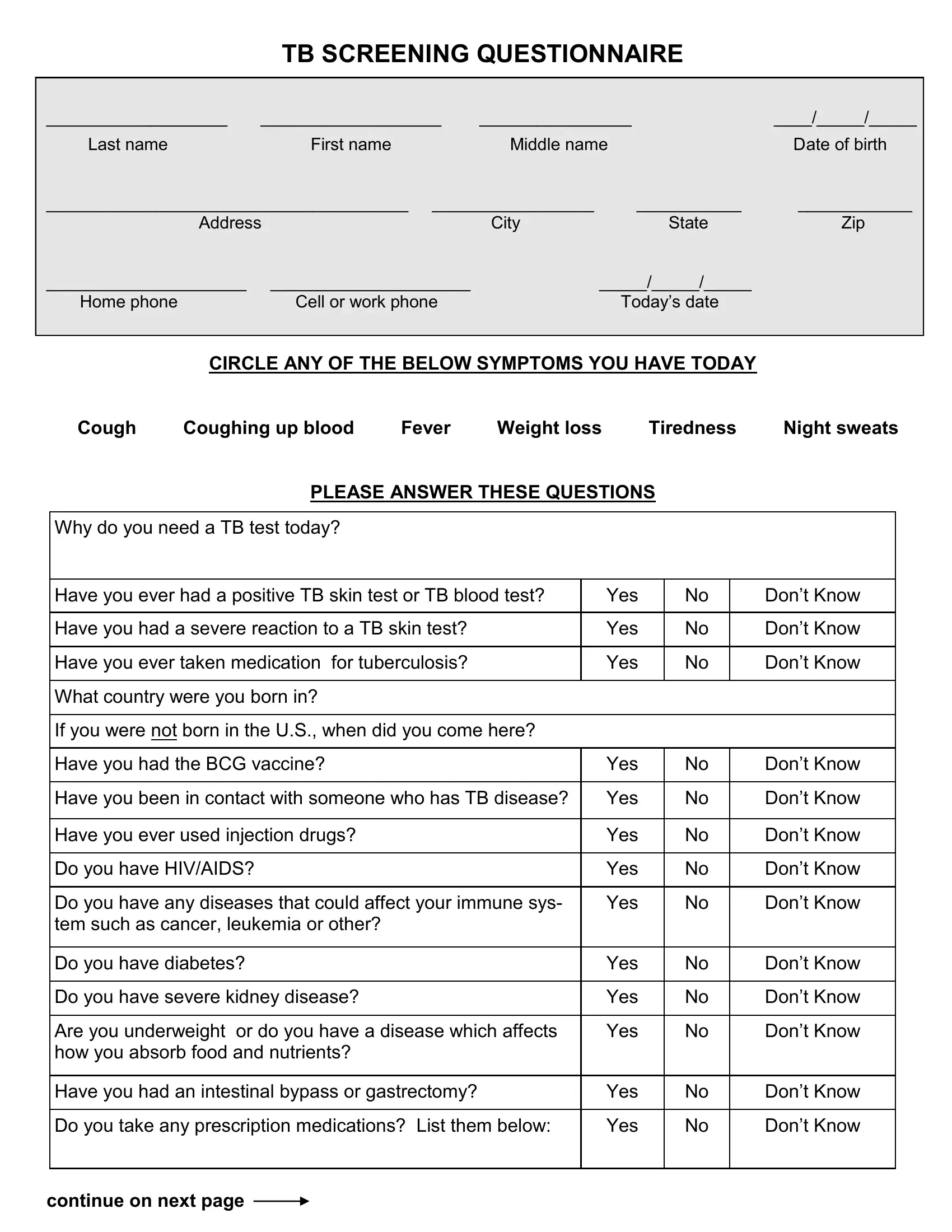
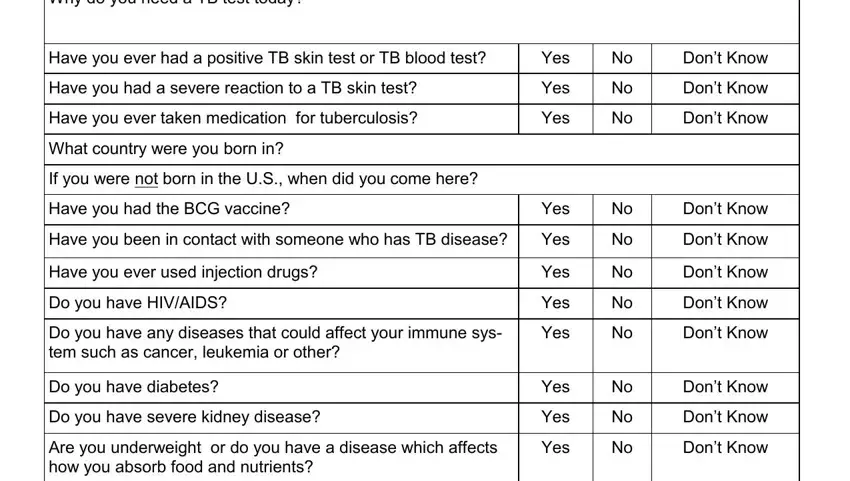
2. Once the last segment is done, you need to add the required details in Why do you need a TB test today, Have you ever had a positive TB, Have you had a severe reaction to, Have you ever taken medication for, What country were you born in, If you were not born in the US, Have you had the BCG vaccine, Yes, Yes, Yes, Yes, Have you been in contact with, Yes, Have you ever used injection drugs, and Do you have HIVAIDS so that you can move on further.
3. This next segment should be relatively simple, Have you had an intestinal bypass, Do you take any prescription, Yes, Yes, Dont Know Dont Know, and continue on next page - all of these blanks will need to be filled in here.

4. The subsequent subsection requires your input in the following areas: First, Name Last CONSENT TO TESTING I, Date, Administration, Name of person giving test, Date and time administered, TST, TST, Location circle, L forearm R forearm, and L forearm R forearm. Make certain to give all required details to go further.
5. While you approach the final sections of this file, there are just a few more points to do. Notably, Location circle, L forearm R forearm, L forearm R forearm, Tuberculin manufacturer, Tuberculin exp date and lot, Administrator signature, Results hours, Date and time read, Number of mm of induration across, Interpretation of reading circle, Positive Negative, Interpreting the TST mm is, HIV infected Recent contacts, and People with fibrotic changes on must all be filled out.
Always be extremely mindful while completing People with fibrotic changes on and Number of mm of induration across, since this is the section in which a lot of people make errors.
Step 3: Ensure your details are right and click on "Done" to proceed further. Try a free trial subscription with us and gain instant access to annual tb screening questionnaire form - download or edit in your FormsPal account page. FormsPal offers secure form editing without personal information record-keeping or any type of sharing. Rest assured that your details are safe with us!