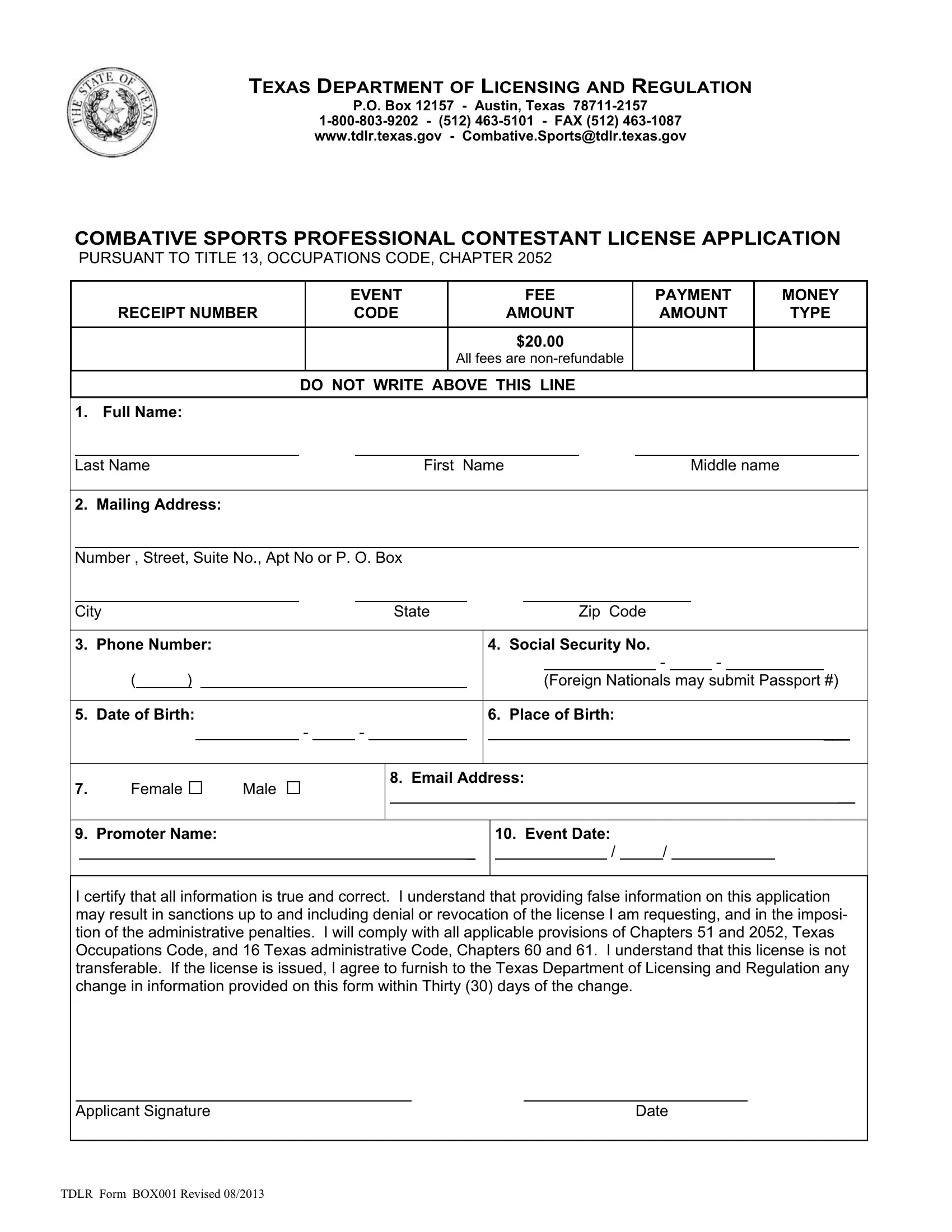
Engaging in combative sports in Texas requires adherence to regulations set forth by the Texas Department of Licensing and Regulation (TDLR), including filing the TDLR Box001 form for a Professional Contestant License Application. This comprehensive document is critical for athletes looking to participate in regulated combative events within the state. It not only facilitates the processing of an event fee but also serves as a detailed application incorporating personal information, medical history, and consent to regulatory compliance. Applicants must provide thorough personal details, from their name and contact information to specific medical data, highlighting the seriousness with which the TDLR takes participant safety and regulatory obedience. Furthermore, the form mandates the attachment of recent medical examination results to ensure the applicant’s fitness for participation. This process underscores the dual focus of the TDLR on both enabling sports events and safeguarding the participants' health and well-being. With non-refundable fees and strict requirements for medical disclosures, including for applicants over 36 years of age, the TDLR Box001 form embodies the rigorous and structured approach of the Texas Department of Licensing and Regulation towards professional combative sports licensing.
| Question | Answer |
|---|---|
| Form Name | Tdlr Form Box001 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | OPHTHALMOLOGIC, bruits, EXTRAOCULAR, COMLICENSED |
TEXAS DEPARTMENT OF LICENSING AND REGULATION
P.O. Box 12157 - Austin, Texas
COMBATIVE SPORTS PROFESSIONAL CONTESTANT LICENSE APPLICATION
PURSUANT TO TITLE 13, OCCUPATIONS CODE, CHAPTER 2052
|
|
|
|
EVENT |
|
FEE |
PAYMENT |
|
MONEY |
|||
|
|
RECEIPT NUMBER |
|
CODE |
|
AMOUNT |
AMOUNT |
|
TYPE |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$20.00 |
|
|
|
|
|
|
|
|
|
|
|
|
All fees are |
|
|
|
|
|
|
|
|
DO NOT WRITE ABOVE THIS LINE |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
Full Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Last Name |
|
|
|
First Name |
Middle name |
|
|
||||
2. |
Mailing Address: |
|
|
|
|
|
|
|
|
|
|
|
Number , Street, Suite No., Apt No or P. O. Box
City |
|
|
|
|
|
|
|
|
|
State |
|
|
Zip Code |
|
|
|
|
|
|
|
|
|
||||||
3. |
Phone Number: |
|
|
|
|
|
|
|
|
4. Social Security No. |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
- |
|
- |
|
|
|
|
||
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
(Foreign Nationals may submit Passport #) |
|||||||||||
5. |
Date of Birth: |
|
|
|
|
|
|
|
|
6. Place of Birth: |
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
- |
|
- |
|
|
|
|
|
|
|
|
|
|
|
___ |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Female □ |
Male □ |
|
|
|
8. Email Address: |
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
__ |
|||||||||||||||
9. |
Promoter Name: |
|
|
|
|
|
|
|
|
|
10. Event Date: |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
_ |
|
|
|
/ |
|
|
/ |
|
|
|
|
|
|
|
|||||
I certify that all information is true and correct. I understand that providing false information on this application may result in sanctions up to and including denial or revocation of the license I am requesting, and in the imposi- tion of the administrative penalties. I will comply with all applicable provisions of Chapters 51 and 2052, Texas Occupations Code, and 16 Texas administrative Code, Chapters 60 and 61. I understand that this license is not transferable. If the license is issued, I agree to furnish to the Texas Department of Licensing and Regulation any change in information provided on this form within Thirty (30) days of the change.
Applicant Signature |
Date |
TDLR FORM BOX001 REVISED 08/2013

APPLICANT NAME (Please print) _____________________________
PROFESSIONAL CONTESTANT'S MEDICAL EXAMINATION - PART 1
TO BE COMPLETED BY A LICENSED MEDICAL DOCTOR ONLY
Forms completed by a physician assistant or a nurse practitioner will NOT be accepted
Medical Allergies ______________________________________________________________________
Are you taking any medication? __ YES __ NO; EXPLAIN _____________________________________
Previous Hospitalization(s) or surgery (Give dates) ______________________________________________
Results of the following blood tests must be attached to this application:
□Hepatitis B surface ANTIGEN
□Hepatitis C ANTIBODY
□HIV ANTIBODY
ALL MEDICAL AND LAB TEST RESULTS MUST BE DATED AND TAKEN
WITHIN THE LAST 6 MONTHS BEFORE THE APPLICATION IS SUBMITTED.
Answer All Questions Below (circle each answer) |
|
|
|
|
|
(A) BLEEDING TENDENCIES |
YES |
NO |
(L) SEIZURES AND CONVULSIONS |
YES |
NO |
(B) DIABETES |
YES |
NO |
(M) ASTHMA |
YES |
NO |
(C) HERNIA |
YES |
NO |
(N) HIGH BLOOD PRESSURE |
YES |
NO |
(D) HEART DISEASE |
YES |
NO |
(O) TUBERCULOSIS |
YES |
NO |
(E) SICKLE CELL DISEASE |
YES |
NO |
(P) MONONUCLEOSIS |
YES |
NO |
(F) KIDNEY DISEASE |
YES |
NO |
(Q) RHEUMATIC FEVER |
YES |
NO |
(G) HEPATITIS |
YES |
NO |
(R) COUGH |
YES |
NO |
(H) SKIN DISEASE |
YES |
NO |
(S) PSYCHIATRIC PROBLEMS |
YES |
NO |
(I) HEADACHES |
YES |
NO |
(T) CONTACT LENSES |
YES |
NO |
(J) JOINT INJURY OR DISLOCATION |
YES |
NO |
(U) NUMBER OF TIMES KO'D |
_______ |
|
(K) CONCUSSION/UNCONSCIOUSNESS |
YES |
NO |
(V) KIDNEY, LUNG, TESTICLE, EYE REMOVED |
YES |
NO |
Do you have any other information concerning your health, past or present, which is NOT COVERED
by the questions above? __________________________________________________________________________________
A PERSON AGE 36 OR OLDER MUST ALSO SUBMIT A FAVORABLE:
EEG (Electroencephalography) AND
EKG (Electrocardiogram)
EXAMINING MD or DO NAME (Please print) _______________________________________________
MEDICAL LICENSE # __________________________________________________________________
(must be licensed in a State, District or Territory of the United States)
ADDRESS _________________________________________________ CITY _______________________
STATE ____________ ZIP ____________ PHONE NUMBER ____________________________________
MD or DO SIGNATURE ________________________________________ DATE ___________________
APPLICANT SIGNATURE |
_____ DATE |
___ |
||
|
|
|
|
|
APPLICANT NAME (Please Print)________________________________ |
|
|||
TDLR FORM BOX001 REVISED 08/2013
PROFESSIONAL CONTESTANT'S MEDICAL EXAMINATION - PART 2
EARS
AUDITORY CANALS |
RIGHT _____ LEFT _______ |
DRUMS |
RIGHT _____ LEFT _______ |
AUDITORY ACUITY FOR CONVERSATIONAL VOICE |
RIGHT _____ LEFT _______ |
NOSE (note deformity, old fractures, deviated septum, other)
__________________________________________________________________
OROPHARYNX
TONSILS ________________ GUM ___________________ TEETH __________________________
TONGUE (record any deviation or tremors) ____________________________________________
NECK (note masses, pulse, thyroid, carotid, bruits, and limitation of motion)
THORAX
LUNGS __________________________________________________________________________
HEART (size, murmurs, arrhythmia) __________________________________________________
HEART RATE ______________________ BLOOD PRESSURE (S) __________ (D) _____________
PULSE RATE _______________________ IMMEDIATELY AFTER 20 HOPS __________________
2 MINUTES AFTER EXERCISE _____________________________________________________________
ABDOMEN
NOTE SCARS _____________________________________________________________________
LIVER, KIDNEY, SPLEEN (enlarged, tender) ___________________________________________
INGUINAL AREA (tenderness, hernia) ________________________________________________
SKIN (note staph infection, cyanosis, hair distribtion____________________________________
LYMPHATIC SYSTEM ___________________________________________________________________
MUSCULOSKELETAL SPINAL SYSTEM (curvature, posture, tenderness, limitation of motion)
__________________________________________________________________
EXTREMITIES (deformity, tenderness, joint mobility) __________________________________________
NEUROLOGICAL
GAIT ________________________________ RHOMBERG ________________________________
FINGER TO NOSE _____________________ KNEE JERKS _______________________________
BICEP JERKS _________________________ BABINSKI __________________________________
BRUDZINSKI _________________________ CRANIAL NERVES __________________________
I hereby certify that I have examined ______________________________________________
(please print applicant’s name)
Date of the exam: ________________ , ________________ ________________
MonthDay Year
I HAVE APPROVED THIS PERSON TO PARTICIPATE IN A COMBATIVE SPORTS EVENT.
MD or DO SIGNATURE ________________________________________ DATE ___________________
APPLICANT SIGNATURE _______________________________________ DATE ___________________
TDLR FORM BOX001 REVISED 08/2013

APPLICANT NAME (Please Print)_________________________
** OPHTHALMOLOGIC MEDICAL EXAM **
Exam with dilation must be done by an OPHTHALMOLOGIST or OPTOMETRIST
EXAMINATION (normal – N; abnormal - X) |
RIGHT EYE |
LEFT EYE |
VISUAL ACUITY |
N _________ |
N ________ |
(WITHOUT CORRECTION) |
|
|
|
F _________ |
F ________ |
EXTERIOR EXAM |
_________ |
________ |
ANTERIOR EXAM |
_________ |
________ |
FUNDI |
_________ |
________ |
EXTRAOCULAR MUSCLES |
_________ |
________ |
VISUAL FIELDS (Confrontation) |
_________ |
________ |
TONOMETRY |
__________ |
_________ |
EXPLAIN ABNORMAL FINDINGS
___________________________________________________________________________
DIAGNOSIS ________________________________________________________________________
____________________________________________________________________________________
I hereby certify that a dilated exam was performed on:_________________________________________
|
|
(please print applicant’s name) |
Date of the exam: ________________ , ________________ ________________ |
||
Month |
Day |
Year |
I HAVE APPROVED THIS PERSON TO PARTICIPATE IN A COMBATIVE SPORTS EVENT.
Ophthalmologist or Optometrist NAME ____________________________________________________
(please print)
LICENSE # _____________________________________________________________________________
(must be licensed in a State, District or Territory of the United States)
ADDRESS _________________________________________________ CITY _______________________
STATE ____________ ZIP ____________ PHONE NUMBER ____________________________________
OPHTHAMOLOGIST or
OPTOMETRIST SIGNATURE _______________________________________ DATE _______________
APPLICANT SIGNATURE _______________________________________ DATE __________________
TDLR FORM BOX001 REVISED 08/2013