
Whenever you wish to fill out h1200 form, there's no need to install any kind of software - just use our PDF editor. FormsPal is devoted to giving you the absolute best experience with our editor by constantly presenting new features and improvements. With all of these improvements, using our editor gets easier than ever! In case you are looking to begin, here's what it requires:
Step 1: Click on the "Get Form" button in the top section of this webpage to access our PDF tool.
Step 2: This editor will give you the opportunity to change your PDF form in a range of ways. Change it by writing your own text, adjust what's already in the PDF, and put in a signature - all readily available!
As for the blanks of this precise document, this is what you want to do:
1. Start filling out your h1200 form with a group of necessary blanks. Note all of the important information and be sure there is nothing overlooked!
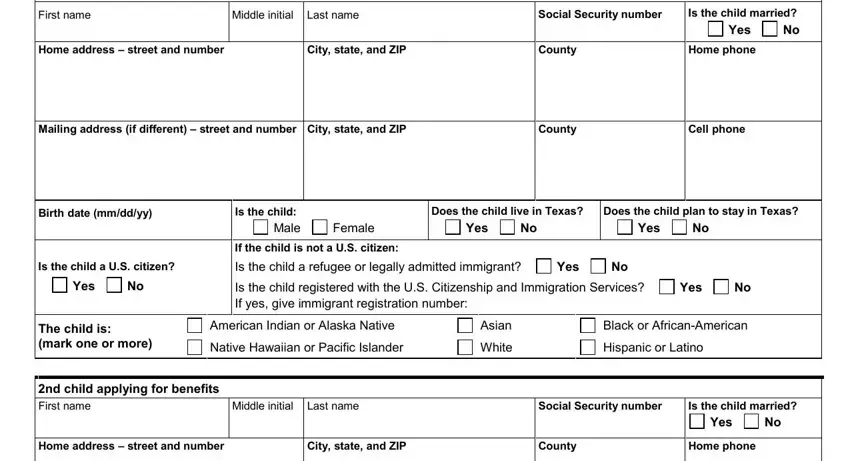
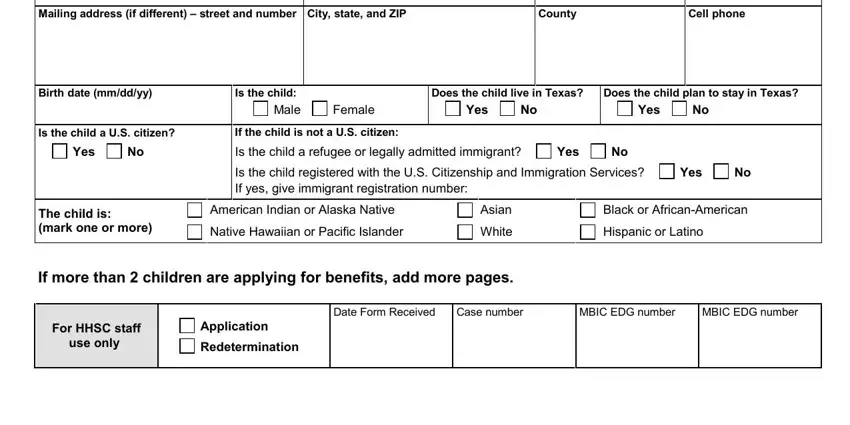
2. Once the last section is done, proceed to enter the applicable information in all these - Mailing address if different, County, Cell phone, Birth date mmddyy, Is the child a US citizen, Yes, Is the child Male, Female, Does the child live in Texas, Yes, Does the child plan to stay in, Yes, If the child is not a US citizen, Is the child a refugee or legally, and Yes.
3. Completing st parent First name, Middle initial Last name, Social Security number optional, Do you live with the child, Yes, Are you Male, Female, Birth date optional, The following questions are about, Do you want this parents employer, Yes, Employers name and address, Gross amount paid before taxes are, How often are you paid once a week, and Yes is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
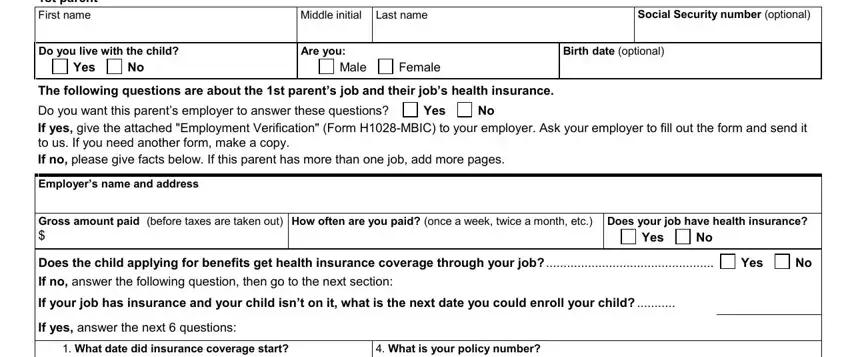
When it comes to Yes and Yes, make certain you double-check them here. Both these are certainly the key ones in this document.
4. The next section requires your attention in the following places: How much do you pay for the, Does your employer pay at least, this is usually a monthly payment, Yes, What is the insurance companys, What is the insurance companys, nd parent First name, Middle initial Last name, Social Security number optional, Do you live with the child, Yes, Are you Male, Female, Birth date optional, and The following questions are about. Ensure that you type in all required info to move onward.
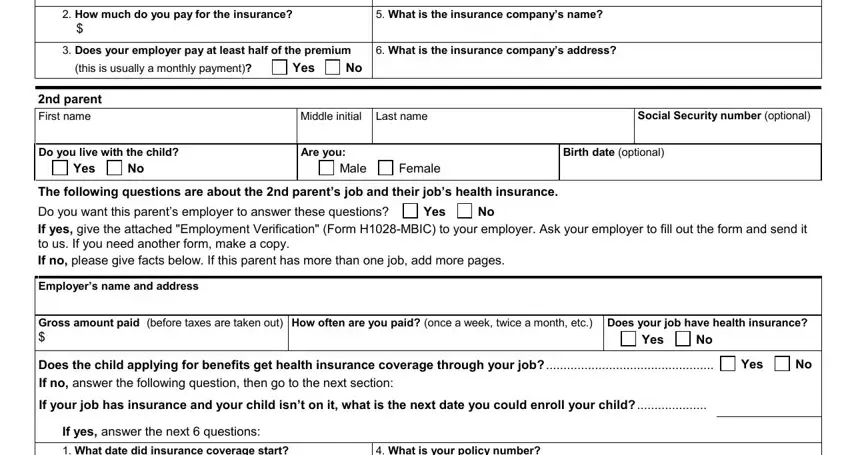
5. As a final point, this final section is what you should finish prior to using the PDF. The blank fields at this point are the next: What date did insurance coverage, What is your policy number, How much do you pay for the, Does your employer pay at least, this is usually a monthly payment, Yes, What is the insurance companys, and What is the insurance companys.

Step 3: Make certain the details are accurate and then simply click "Done" to progress further. Join us right now and instantly use h1200 form, prepared for download. Every single modification made is handily preserved , making it possible to customize the form at a later time as required. We do not share any details that you use when filling out documents at our website.