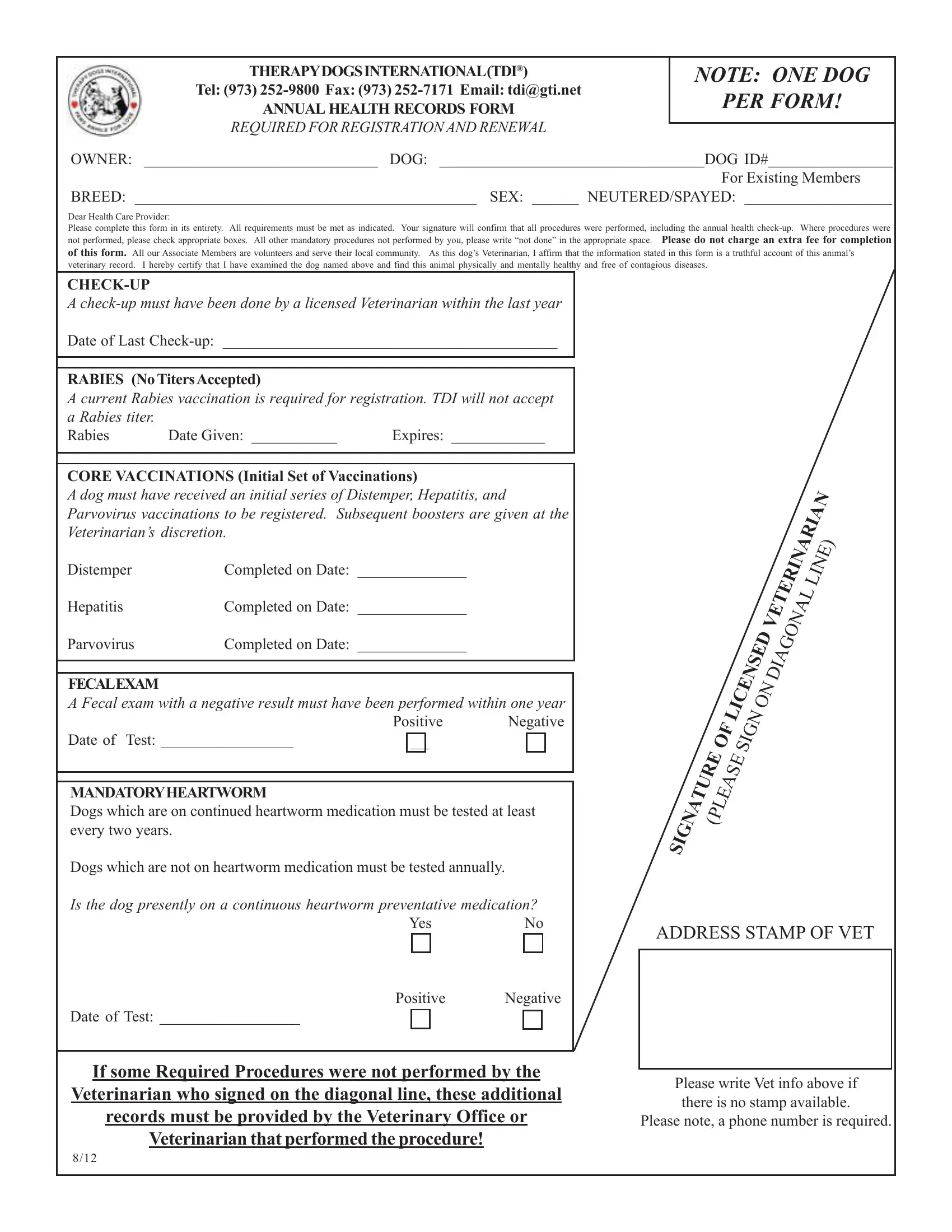
THERAPYDOGSINTERNATIONAL(TDI®)
Tel: (973) 252-9800 Fax: (973) 252-7171 Email: tdi@gti.net
ANNUAL HEALTH RECORDS FORM
REQUIRED FOR REGISTRATIONAND RENEWAL
OWNER: ______________________________ DOG: __________________________________DOG ID#________________
For Existing Members
BREED: ____________________________________________ SEX: ______ NEUTERED/SPAYED: ___________________
Dear Health Care Provider:
Please complete this form in its entirety. All requirements must be met as indicated. Your signature will confirm that all procedures were performed, including the annual health check-up. Where procedures were not performed, please check appropriate boxes. All other mandatory procedures not performed by you, please write “not done” in the appropriate space. Please do not charge an extra fee for completion of this form. All our Associate Members are volunteers and serve their local community. As this dog’s Veterinarian, I affirm that the information stated in this form is a truthful account of this animal’s veterinary record. I hereby certify that I have examined the dog named above and find this animal physically and mentally healthy and free of contagious diseases.
CHECK-UP
A check-up must have been done by a licensed Veterinarian within the last year
Date of Last Check-up: ___________________________________________
RABIES (NoTitersAccepted)
A current Rabies vaccination is required for registration. TDI will not accept
a Rabies titer. |
|
|
Rabies |
Date Given: ___________ |
Expires: ____________ |
CORE VACCINATIONS (Initial Set of Vaccinations)
A dog must have received an initial series of Distemper, Hepatitis, and Parvovirus vaccinations to be registered. Subsequent boosters are given at the Veterinarian’s discretion.
Distemper |
Completed on Date: ______________ |
Hepatitis |
Completed on Date: ______________ |
Parvovirus |
Completed on Date: ______________ |
FECALEXAM
A Fecal exam with a negative result must have been performed within one year
Positive Negative
Date of Test: _________________
MANDATORYHEARTWORM
Dogs which are on continued heartworm medication must be tested at least every two years.
Dogs which are not on heartworm medication must be tested annually.
Is the dog presently on a continuous heartworm preventative medication?
Yes No
Positive Negative
Date of Test: __________________
If some Required Procedures were not performed by the Veterinarian who signed on the diagonal line, these additional records must be provided by the Veterinary Office or Veterinarian that performed the procedure!
|
|
|
VETERINARIAN |
|
|
|
LINE) |
|
LICENSEDON |
DIAGONAL |
|
|
OF |
|
SIGN |
|
SIGNATURE (PLEASE |
|
|
ADDRESS STAMP OF VET
Please write Vet info above if there is no stamp available.
Please note, a phone number is required.
Therapy Dogs International (TDI®)
Inoculation Statement for Dogs Vaccinated by
Someone Other Than a Veterinarian
I, |
, certify that ____________________ |
|
Owner/Handler’s Name (PLEASE PRINT) |
Dog’s Name |
has received all vaccinations listed below on the indicated dates. This dog also has a current Rabies vaccination.
Rabies vaccination MUST be performed by a veterinarian. An initial series of all Core Vaccinations specified on the front of this form (Distemper, Hepatitis, Parvovirus) must be given. Subsequent boosters and/or titers for Core Vaccinations should be given following a schedule recommended by your Veterinarian.
LIST ALL VACCINATIONS
Vaccine (s)DatePlaceVaccinated by
____________________________________________________________________________________________________
Vaccine (s) |
Date |
Place |
Vaccinated by |
|
|
|
|
Vaccine (s) |
Date |
Place |
Vaccinated by |
|
|
|
|
Vaccine (s) |
Date |
Place |
Vaccinated by |
|
|
|
|
|
Vaccine (s) |
Date |
Place |
Vaccinated |
by |
|
|
|
|
|
Vaccine (s) |
Date |
Place |
Vaccinated |
by |
Please include a copy of invoices that show you have purchased the vaccines listed above for dogs
applying for registration with TDI®
We cannot process your application without the mandatory invoices or labels.
I hereby certify that I, __________________________________________________________________________________
Signature of Vaccinator |
Vaccinator’s Name (PLEASE PRINT) |
have given the vaccines to the dog noted above and I take full responsibility. |
|
____________________________________________________________________________________________________
Vaccinator’s Address and Telephone Number (PLEASE PRINT)DatePlace
_____________________________________________________________________________________________________________________________
Owner/Handler’s SignatureDate
Copies of this form may be made ONLY for Therapy Dogs International use.
8/12