TRICARE Reserve Select (TRS) / TRICARE Retired Reserve (TRR)
Premium Payment Credit Card & EFT Authorization Form
Select One: |
|
One-time Payment |
Enroll to Auto Monthly Payment |
Disenroll from Auto Payments |
|
|
|
|
|
By signing this form you are authorizing International SOS Assistance, Inc. as applicable, to initiate debit/credit card or EFT charges (and/or corrections to previous debits/charges) from your account with the financial institution identified on this form for payment of TRS/TRR premiums. A fee of $20 may be applied for insufficient EFT funds.
Important note for auto monthly payments: Payment of any past due amount is required to set up an automated monthly payment account. If you have any unpaid balance over 30 days, it will be charged / debited before new automatic payments occur. By signing this form you are authorizing International SOS Assistance Inc., as applicable, to initiate debit/credit charges (and/or corrections to previous debits/charges) from my account with the financial institution identified by me on this form for payment of my TRS/TRR premiums. This authorization will remain in effect until I provide written notice revoking the authorization to International SOS Assistance Inc. at least 10 days before my account is to be debited/charged.
Section I. Beneficiary information
TRS/TRR Sponsor Name: _____________________________________________________________
DEERS Family ID / SSN: _____________________________________________________________
Mailing address: ____________________________________________________________________
City, state, ZIP: _____________________________________________________________________
Daytime phone number: __________________ E-mail: _____________________________________
Section II. Select an option below and complete the section.

 Option #1 - Financial Institution Information for Electronic Fund Transfer (EFT)
Option #1 - Financial Institution Information for Electronic Fund Transfer (EFT)
Type of account: |
Checking |
Savings |
Bank routing/transfer number: _____________________________________________
Bank account number ___________________________________________________
Name of financial institution: _______________________________________________
Name(s) on bank account: ________________________________________________
Branch address, city, state, ZIP: ____________________________________________
Branch telephone number: ________________________________________________
Option #2 - Credit card payments |
|
Type of account: |
Visa |
MasterCard |
Cardholder name: _______________________________________________________
Cardholder billing address: ________________________________________________
City: _____________ State: _______ ZIP: ________ Country: _________
Credit Card Number: _____________________________________________________
CVV/CVV2:__________ Expiration date: ________________
Section III. Authorized signature
By signing this form, you are authorizing International SOS Assistance, Inc. to process the request as completed above.
_____________________________________________________________
SignatureDate
________________________________________________
Print Name
(CONT.)
FORM INSTRUCTIONS:
Use this form if you would like to initiate or discontinue a TRS/TRR premium payment using your credit/debit card or and electronic fund transfer from your bank account. Forms will be process within 10 days of receipt. Upon receipt of this form International SOS will process all outstanding charges (if any) due for your TRS/TRR premium program balance.
Section I. – Beneficiary Information
Complete TRS/TRR Sponsor account information. Please do not leave anything blank. Please provide a phone number where we can reach you if we need your assistance in processing the information you provided on this form.
Section II. - Choose payment option
Complete section for EFT (Electronic Funds Transfer) for checking or savings account debits, or the Credit Card section for Visa or MasterCard payments.
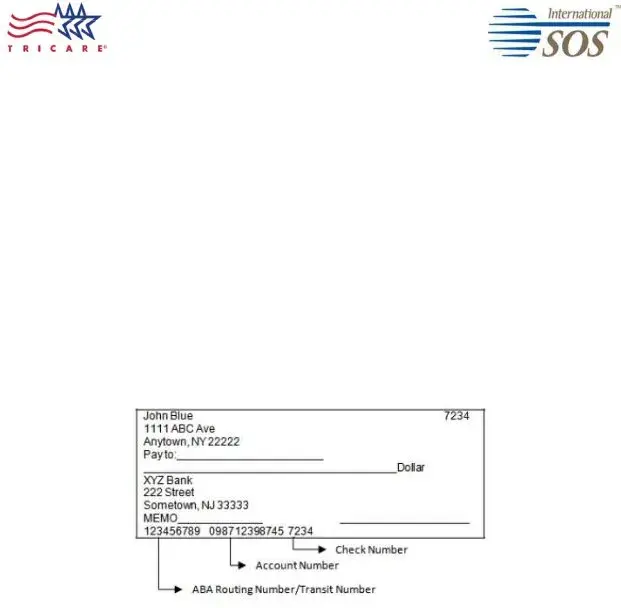
Option #1 – Electronic Fund Transfer (EFT) from your Checking or Savings Account
For EFT, enclose a blank check mark “VOID.” If you prefer not to attach a voided check, you must provide your bank account number and routing/transit number (see below). The example provided below is for US bank accounts. If you are using non-US financial institution, please contact your financial institution for assistance in obtaining your required information for this form.
Option #2 - Credit card payment by Visa and MasterCard
Credit card payments are only offered for Visa or MasterCard. For your added security, we ask that you provide your credit card CVV code. The CVV is a three- or four-digit value printed on the back of your card located near your signature strip.
Section III. Authorized signature (If you are disenrolling from auto monthly payments, select “Disenroll from auto payments” and sign in Section III)
HOW TO SUBMIT FORM:
Submit a completed copy of page 1 of this form via one of the options below
Mail to: International SOS Assistance, Inc
Attention: TRS/TRR Accounts Receivable
PO Box 11689
Philadelphia, PA 19116
Fax to: +1 215-354-2340
(CONT.)
PRIVACY ACT STATEMENT
AUTHORITY: 10 U.S.C. 1079 and 1086, 32 U.S.C. Chapter 17; 32 CFR 199.17; 45 CFR Parts 160 and 164, Health Insurance Portability and Accountability Act (HIPAA) Privacy and Security Rules; and E.O. 9397 (SSN), as amended.
PRINCIPAL PURPOSE(S): To obtain information necessary to permit individuals to initiate or discontinue premium payments via electronic funds transfers from your banking or credit account.
ROUTINE USE(S): In addition to those disclosures generally permitted under 5 U.S.C. 552a(b) of the Privacy Act of 1974, as amended, these records may specifically be disclosed outside the Department of Defense as a routine use pursuant to 5 U.S.C. 552a(b)(3) as follows: to the Departments of Health and Human Services, Homeland Security, and Veterans Affairs, and to other Federal, State, local, or foreign government agencies, and to private business entities, including entities under contract with the Department of Defense and individual providers of care, on matters relating to eligibility, claims pricing and payment, fraud, program abuse, utilization review, quality assurance, peer review, program integrity, third-party liability, coordination of benefits, and civil or criminal litigation.
DISCLOSURE: Voluntary; however, failure to provide information may result in the denial of premium payments, fees for insufficient funds, or disruption in your coverage due to non-payment.