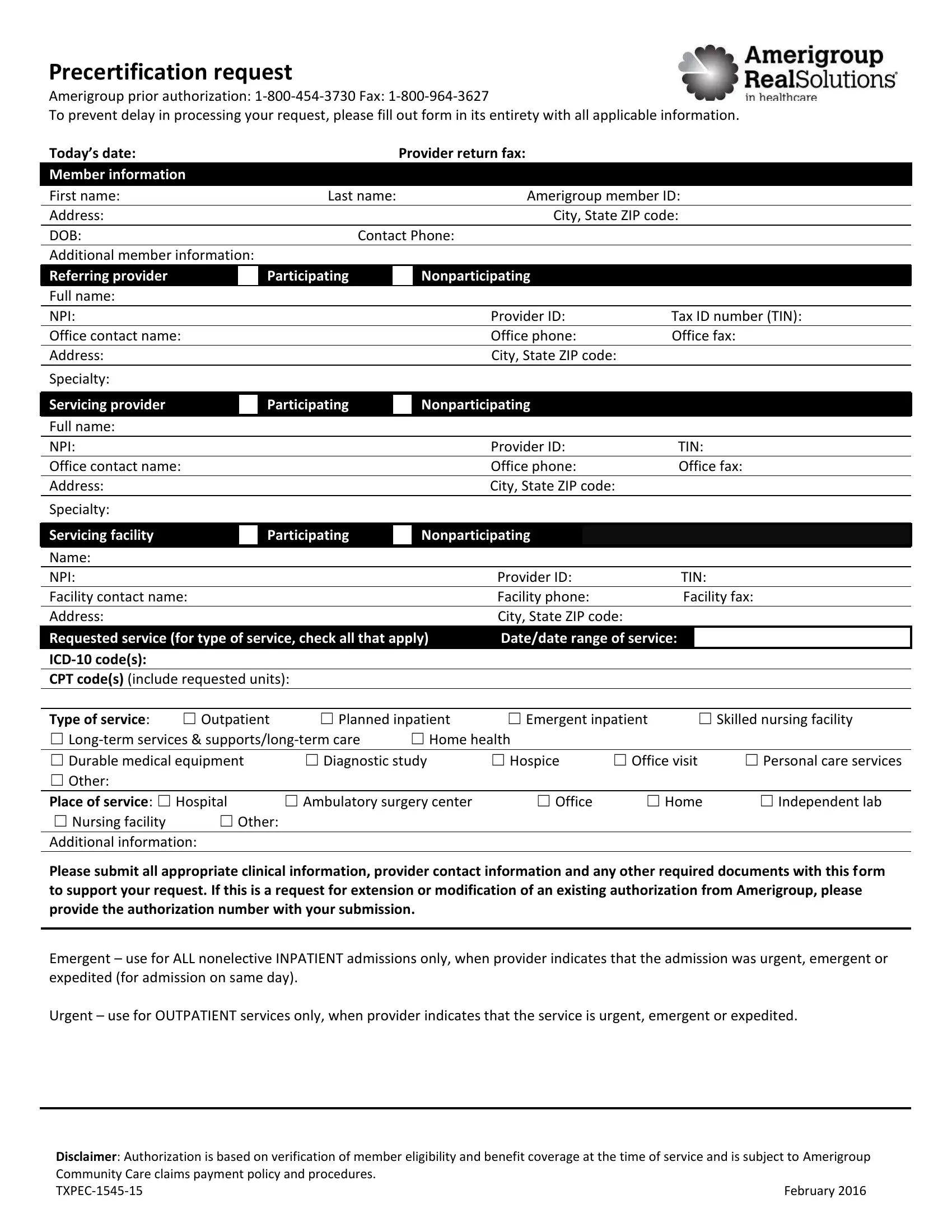
In the healthcare sector, navigating the process of obtaining prior authorization can often seem like a daunting task for providers. The Txpec form, specifically designed for Amerigroup, serves as a critical tool in facilitating this complex process. At its core, the form functions as a precertification request, ensuring that the necessary approvals are acquired before proceeding with patient care. Providers are required to meticulously fill out the form, providing comprehensive member and service information to avoid any delays in processing. The form encompasses a range of crucial details, including both the requesting and servicing provider's information, member details, and the specifics of the requested service, such as the type of service, dates, and pertinent codes (ICD-10 and CPT). Additionally, the form distinguishes between different service settings, including outpatient and inpatient services, among others, making it an essential document for various healthcare scenarios. Moreover, the inclusion of a section for additional clinical information underscores the importance of thorough documentation in supporting the request. As such, properly completing the Txpec form is a vital step in ensuring patients receive timely access to care while adhering to Amerigroup's authorization procedures, outlined clearly with contact numbers and a disclaimer at the form's conclusion.
| Question | Answer |
|---|---|
| Form Name | Txpec Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form precertification request amerigroup, txpec, precertification request get, contact authorization amerigroup get |
Precertification request
Amerigroup prior authorization:
To prevent delay in processing your request, please fill out form in its entirety with all applicable information.
Today’s date: |
Provider return fax: |
|
Member information |
|
|
First name: |
Last name: |
Amerigroup member ID: |
|
|
|
Address: |
|
City, State ZIP code: |
|
|
|
DOB: |
Contact Phone: |
|
|
|
|
Additional member information: |
|
|
Referring provider
Participating
Nonparticipating
Full name:
NPI: |
|
|
|
|
|
|
|
|
|
Provider ID: |
|
Tax ID number (TIN): |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Office contact name: |
|
|
|
|
|
|
|
|
|
Office phone: |
|
Office fax: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
City, State ZIP code: |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Servicing provider |
|
|
|
Participating |
|
|
|
Nonparticipating |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Full name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
NPI: |
|
|
|
|
|
|
|
|
|
Provider ID: |
|
TIN: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Office contact name: |
|
|
|
|
|
|
|
|
|
Office phone: |
|
Office fax: |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Address: |
|
|
|
|
|
|
|
|
|
City, State ZIP code: |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Specialty: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Servicing facility |
|
|
|
Participating |
|
|
|
Nonparticipating |
|
|
|
|
|
|
||
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NPI: |
|
|
|
|
|
|
|
|
|
Provider ID: |
|
TIN: |
|
||||
Facility contact name: |
|
|
|
|
|
|
|
Facility phone: |
|
Facility fax: |
|||||||
Address: |
|
|
|
|
|
|
|
|
|
City, State ZIP code: |
|
|
|
||||
|
Requested service (for type of service, check all that apply) |
Date/date range of service: |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
CPT code(s) (include requested units): |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
||||||||||||
Type of service: |
☐ Outpatient |
☐ Planned inpatient |
☐ Emergent inpatient |
|
☐ Skilled nursing facility |
||||||||||||
☐ |
☐ Home health |
|
|
|
|
||||||||||||
☐ Durable medical equipment |
|
|
☐ Diagnostic study |
☐ Hospice |
☐ Office visit |
☐ Personal care services |
|||||||||||
☐ Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Place of service: ☐ Hospital |
|
|
☐ Ambulatory surgery center |
☐ Office |
☐ Home |
☐ Independent lab |
|||||||||||
|
☐ Nursing facility |
☐ Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
Additional information:
Please submit all appropriate clinical information, provider contact information and any other required documents with this form to support your request. If this is a request for extension or modification of an existing authorization from Amerigroup, please provide the authorization number with your submission.
Emergent – use for ALL nonelective INPATIENT admissions only, when provider indicates that the admission was urgent, emergent or expedited (for admission on same day).
Urgent – use for OUTPATIENT services only, when provider indicates that the service is urgent, emergent or expedited.
Disclaimer: Authorization is based on verification of member eligibility and benefit coverage at the time of service and is subject to Amerigroup
Community Care claims payment policy and procedures. |
|
February 2016 |