
REAPPLICATION can be filled out online in no time. Simply open FormsPal PDF tool to accomplish the job promptly. Our tool is continually evolving to give the best user experience possible, and that's thanks to our commitment to continual development and listening closely to user feedback. Here is what you'd want to do to get going:
Step 1: Access the form inside our editor by pressing the "Get Form Button" in the top part of this page.
Step 2: The editor provides the capability to work with almost all PDF forms in a range of ways. Transform it by writing personalized text, adjust what is already in the file, and place in a signature - all when it's needed!
With regards to the blank fields of this specific document, this is what you should consider:
1. Start completing the REAPPLICATION with a group of major fields. Consider all of the necessary information and ensure nothing is neglected!
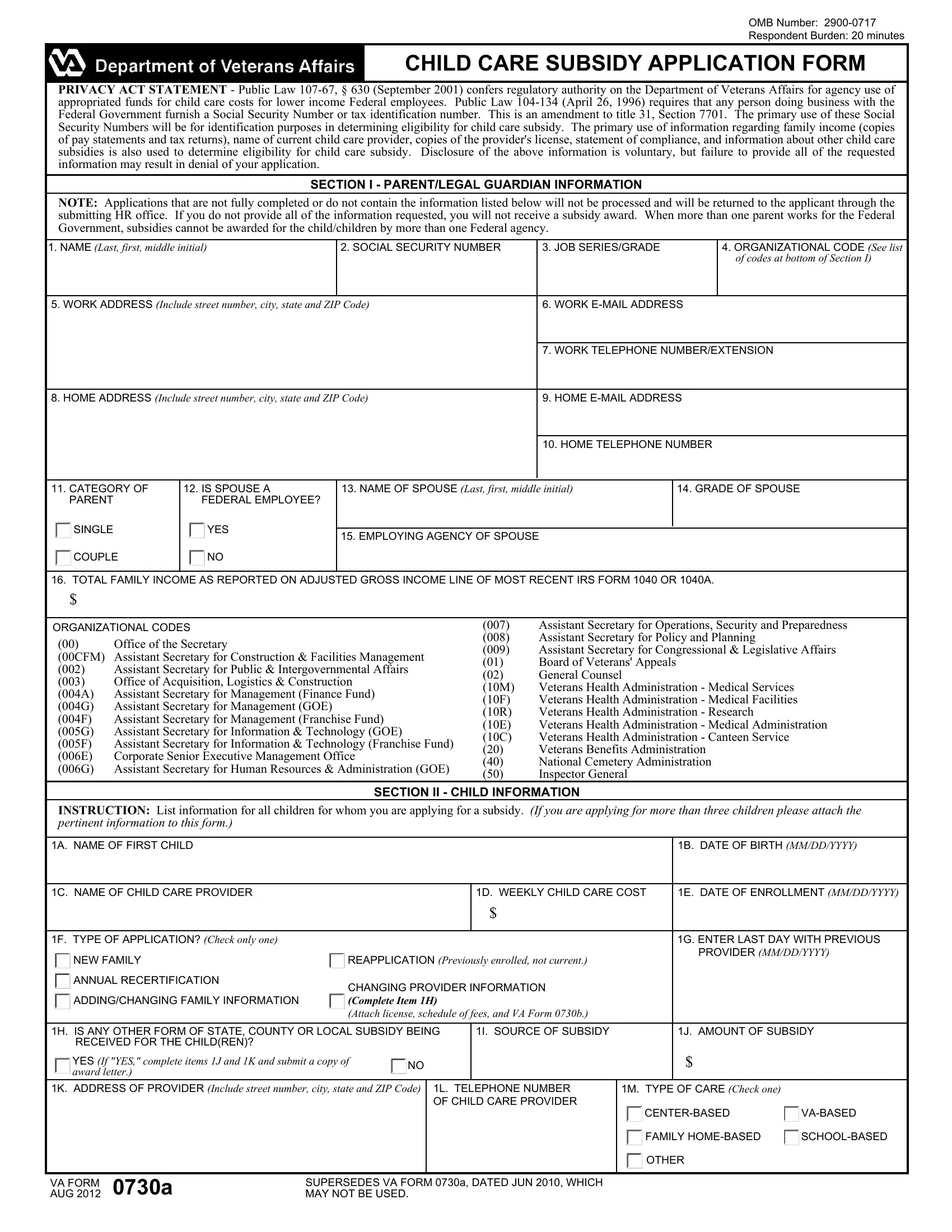
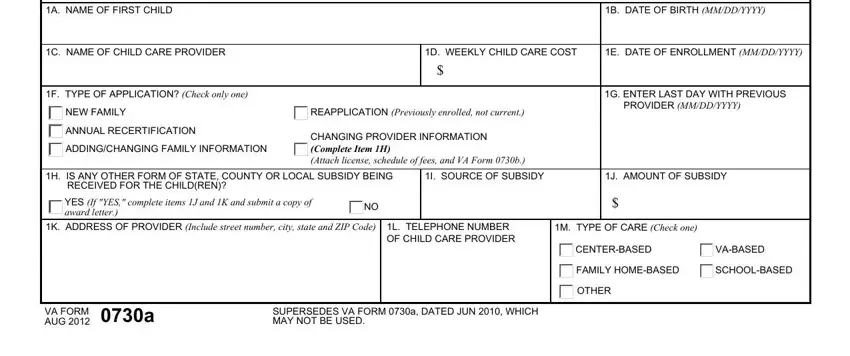
2. Just after the previous array of fields is completed, go on to enter the relevant details in these: A NAME OF FIRST CHILD, B DATE OF BIRTH MMDDYYYY, C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, REAPPLICATION Previously enrolled, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, I SOURCE OF SUBSIDY, and J AMOUNT OF SUBSIDY.
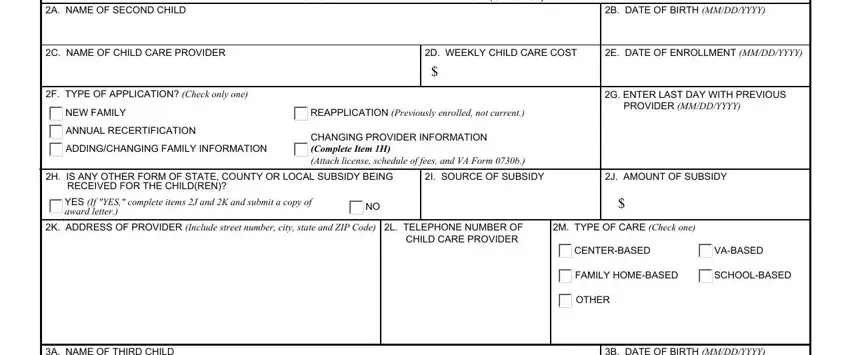
3. Completing A NAME OF SECOND CHILD, B DATE OF BIRTH MMDDYYYY, SECTION II CHILD INFORMATION, C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, REAPPLICATION Previously enrolled, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, and YES If YES complete items J and K is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
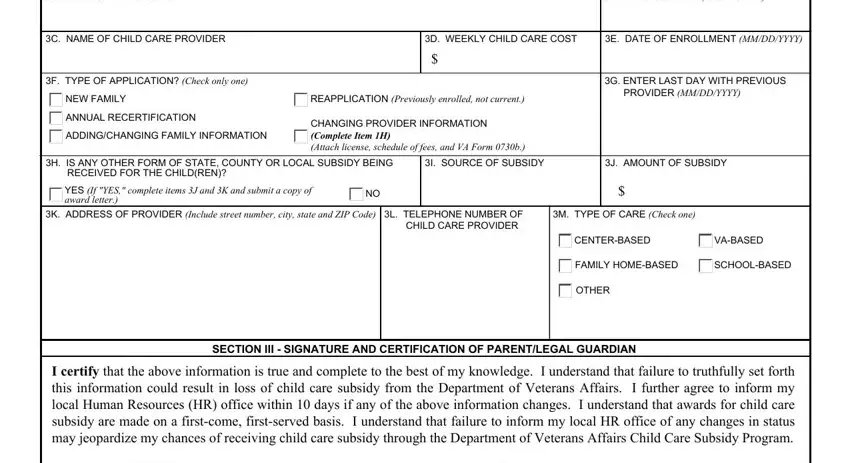
4. Now proceed to this next portion! In this case you've got all these A NAME OF THIRD CHILD, B DATE OF BIRTH MMDDYYYY, C NAME OF CHILD CARE PROVIDER, D WEEKLY CHILD CARE COST, E DATE OF ENROLLMENT MMDDYYYY, F TYPE OF APPLICATION Check only, NEW FAMILY, REAPPLICATION Previously enrolled, ANNUAL RECERTIFICATION, ADDINGCHANGING FAMILY INFORMATION, CHANGING PROVIDER INFORMATION, G ENTER LAST DAY WITH PREVIOUS, H IS ANY OTHER FORM OF STATE, I SOURCE OF SUBSIDY, and J AMOUNT OF SUBSIDY blanks to fill out.
Regarding E DATE OF ENROLLMENT MMDDYYYY and F TYPE OF APPLICATION Check only, ensure that you do everything correctly here. These two are definitely the most important ones in this page.
Step 3: Confirm that your details are right and simply click "Done" to finish the process. Sign up with us now and easily gain access to REAPPLICATION, set for downloading. Every modification you make is conveniently preserved , which means you can change the document later on as required. At FormsPal, we do our utmost to guarantee that all your information is stored protected.