You'll find nothing complicated in relation to completing the 10 10ezr online if you use our tool. By following these clear steps, you can receive the ready PDF document in the minimum time frame feasible.
Step 1: The initial step will be to pick the orange "Get Form Now" button.
Step 2: So you are on the file editing page. You can enhance and add text to the file, highlight words and phrases, cross or check particular words, include images, sign it, erase unnecessary fields, or eliminate them altogether.
The PDF file you wish to fill in will consist of the following areas:
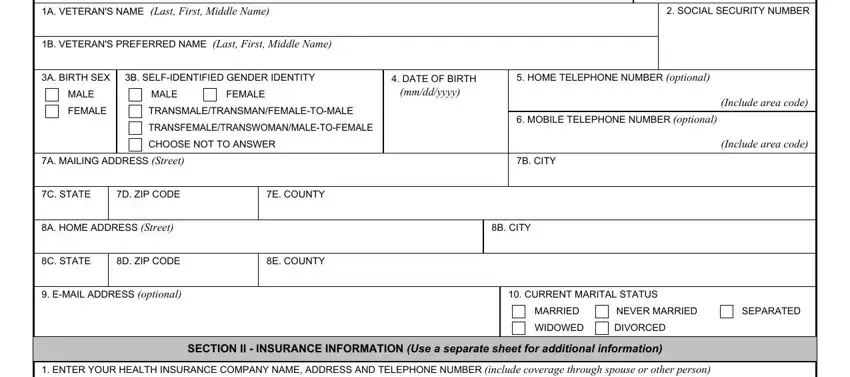
Fill in the Federal law provides criminal, SOCIAL SECURITY NUMBER, B VETERANS PREFERRED NAME Last, A BIRTH SEX, B SELFIDENTIFIED GENDER IDENTITY, MALE, MALE, FEMALE, DATE OF BIRTH mmddyyyy, HOME TELEPHONE NUMBER optional, FEMALE, TRANSMALETRANSMANFEMALETOMALE, TRANSFEMALETRANSWOMANMALETOFEMALE, CHOOSE NOT TO ANSWER, and MOBILE TELEPHONE NUMBER optional space using the details asked by the software.
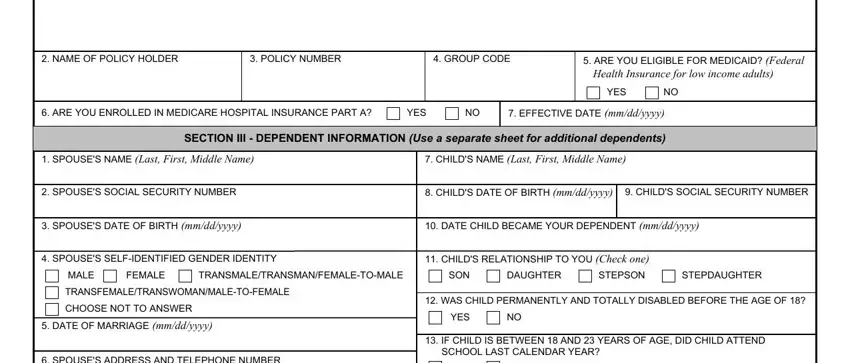
You should be required some essential details so you can fill up the NAME OF POLICY HOLDER, POLICY NUMBER, GROUP CODE, ARE YOU ELIGIBLE FOR MEDICAID, Health Insurance for low income, YES, ARE YOU ENROLLED IN MEDICARE, YES, EFFECTIVE DATE mmddyyyy, SPOUSES NAME Last First Middle, CHILDS NAME Last First Middle Name, SECTION III DEPENDENT INFORMATION, SPOUSES SOCIAL SECURITY NUMBER, CHILDS DATE OF BIRTH mmddyyyy, and CHILDS SOCIAL SECURITY NUMBER section.
The SPOUSES ADDRESS AND TELEPHONE, YES, EXPENSES PAID BY YOU FOR YOUR, VOCATIONAL REHABILITATION OR, IF YOUR SPOUSE OR DEPENDENT CHILD, YES, VA FORM EZR JUL, HEC, PAGE OF, and REMEMBER TO SIGN AND DATE THE FORM box is where both sides can insert their rights and responsibilities.
Look at the areas HEALTH BENEFITS UPDATE FORM, VETERANS NAME Last First Middle, SOCIAL SECURITY NUMBER, SECTION IV PREVIOUS CALENDAR YEAR, VETERAN, SPOUSE, CHILD, GROSS ANNUAL INCOME FROM, etc EXCLUDING INCOME FROM YOUR, NET INCOME FROM YOUR FARM RANCH, LIST OTHER INCOME AMOUNTS eg, pension interest dividends, SECTION V PREVIOUS CALENDAR YEAR, TOTAL NONREIMBURSED MEDICAL, and AMOUNT YOU PAID LAST CALENDAR and thereafter fill them out.
Step 3: Once you've selected the Done button, your form will be ready for export to any kind of device or email you specify.
Step 4: In avoiding probable forthcoming problems, make sure you get at least two copies of any form.
