NOTE: INSTRUCTIONS ARE WRITTEN FOR A MULTI-PART FORM. PRINT ADDITIONAL COPIES AS NECESSARY
DENTAL RECORD AUTHORIZATION AND
INVOICE FOR OUTPATIENT SERVICES
PART I - EXAMINATION PROCEDURE INSTRUCTIONS FOR THE PARTICIPATING FEE DENTIST
1.Examination Authorization. The Department of Veterans Affairs (VA) has authorized this veteran to choose a general practitioner who will complete a thorough oral examination and treatment plan. The VA must be apprised of the veteran's current dental needs so as to make a determination of the extent and type of treatment to be authorized. The allowable fees for radiographs and examination have been indicated in Item 14 on page 3 of this form. The fee for radiographs is based on a full mouth series. This is a basic requirement when no diagnostically usable radiograph record exists relating to a complete dentition. In a circumstance where depleted dentition or edentulous status exists, the requirement for radiographs should be modified by the examining dentist. Any modification from a full mouth series should be annotated by specifying the radiographs actually exposed. The fee will be adjusted, accordingly, by the VA. On subsequent examinations, only radiographs necessary for proper diagnosis and treatment should be taken. Where pre-existing radiographs will serve to satisfactorily augment a thorough clinical evaluation, the pre-printed entry in Item 9 should be crossed out and initiated by the examining dentist.
WHEN IS ITEM 11 COMPLETED? WHICH ITEM AUTHORIZES TREATMENT?
2.Inappropriate selection of fee dentist. If you are a specialist, your practice is restricted to a specialty, or you are currently on active military duty and engaged in part-time private practice, the veteran has made an inappropriate selection of a fee dentist. (VA is prohibited from making payment of fees to a member of the military services.) Return this authorization and allied papers to the veteran and clarify that a Civilian General Practice Dentist must be chosen for examination and treatment plan purposes. If the veteran needs assistance, the Chief of Dental Service at the VA issuing office may be contacted.
3.Use of form. VA Form 10-2570d will serve for examination record, treatment recommendations, record of treatment and invoice for services provided. When you receive the carbon-interleafed VA Form 10-2570d, please keep all copies together. Entries must be made with a typewriter or ball point pen only. Use heavy pressure with a ball point pen. Inspect the last copy to see if all entries have been recorded legibly. Supply all data requested in Items 2 through 5. Be certain to include your telephone number (including area code) in Item 2A.
4.Examination authorized. The examination authorization is your authority to proceed with radiographs and examination only. You may not proceed with definitive dental care for your veteran patient. Payment will not be made for unauthorized treatment. The only exception is for limited EMERGENCY dental care. To obviate an emergency situation, care which is needed at the time of the examination (relief of pain, etc.) can be provided. However, the VA office (shown in Item 1) issuing this authorization must be notified of the details and treatment within 15 days or there is no authority to make payment for these emergency services.
5.Dental examination. Chart all missing teeth in Item 6. Enter the date examination was conducted and radiographs were taken in Item
10opposite the appropriate pre-printed entries in Item 9. During the examination, take care to discuss options and not commit to any specific treatment plan. If there are significant differences between what VA considers reasonable and appropriate and the proposed treatment plan, VA may reexamine the veteran prior to treatment authorization to determine a treatment plan that provides a satisfactory resolution of needs and is compatible with cost containment measures. List all treatment recommendations under Items 7, 8 and 9. Types of abutments and pontics for fixed partial dentures must be stipulated and teeth to be clasped for removable partial dentures must be specified. Enter your usual and customary fee for each line entry under Item 12. Enter statements in Item 13 (Remarks) which will further clarify data under Item 9. Please identify specific teeth which the veteran states were extracted while he was in active military service. Details as to appropriate dates and places of extractions are necessary to determine if replacements can be authorized. When all appropriate entries have been completed, return the packet along with the patient's radiographs to the issuing office (shown in Item 1) for treatment authorization.
6.Requirement to review radiographs. The VA outpatient dental care program operates under legal restriction and, with few exceptions, only those dental conditions determined to be "service-incurred" may be corrected at Government expense. Therefore, it is necessary that treatment recommendations and radiographs be returned to the issuing office (Item 1) for determination of the extent of allowable treatment at VA expense and establishment of authorized fees for these services. Radiographs will be returned to you with the treatment authorization and may be retained by you for your records.
7.Time limitation. There is a time limitation indicated in Item 19. Examination should be completed and findings returned by this date. If veteran does not respond for examination, return the authorization to the issuing office. If there is a good reason an extension of time is required, contact the issuing office (Item 1) for an extension of the time limitation.
8.Payment for Services. Payment for examination and treatment will be made following completion or termination of treatment.
9.Precaution. There may be instances in which recently discharged veterans will report directly to your office requesting that certain dental treatment initiated by the Military during service be completed at Government expense. While it is possible that such veterans, after making application, may be determined eligible for treatment, VA will not be responsible for dental services provided prior to the date treatment is appropriately authorized.
VA FORM |
10-2570D DENTIST: NO PAYMENT WILL BE MADE UNLESS PRE-AUTHORIZED BY VA |
Instructions |
MAR 2008 (R) |

NOTE: INSTRUCTIONS ARE WRITTEN FOR A MULTI-PART FORM. PRINT ADDITIONAL COPIES AS NECESSARY
PART II - TREATMENT PROCEDURE INSTRUCTIONS FOR THE PARTICIPATING FEE DENTIST
1.Treatment Authorization. The Department of Veterans Affairs (VA) has authorized all dental treatment recommended under Item 9 which has not been lined out. The fees specified in Item 12 are approved unless changed in Item 14. Your acceptance of the treatment authorization constitutes a contract to provide the authorized services for the approved fees, as payment in full. DO NOT request the veteran to pay any difference between the fees authorized and your usual customary fees. If you are unable to provide the services for the fees specified, the authorization should be promptly returned to the VA issuing office shown in Item 1. There is no objection to making separate arrangements with the veteran for any need service which legally the VA is unable to authorize.
2.Treatment. When services indicated under Item 9 have been provided, enter the date each service was completed under Item 10. This dated entry in Item 10 will constitute a validation of the service provided by you and claim for payment of said service. When all treatment has been completed, remove the third copy of the form for your records and return the remaining packet to the authorizing office for payment. No separate invoice or letterhead is necessary. In order to avoid any misunderstanding concerning fraud, submission of the completed form to the VA should not take place until all the treatment for which claim is being made has been provided.
3.Change in Treatment Plan by VA. The VA is the primary provider of dental care for VA beneficiaries and not a third-party carrier. Treatment cases which are beyond the VA's capability to provide care in timely fashion are referred to fee dentists as alternate providers. Consequently, there is need for consistency between the type and amount of care provided by the VA and that provided by private dentists. If on review of your treatment plan, the VA disagrees with either of these factors, the Chief of Dental Service will contact you to discuss the change or it will be noted on the VA Form 10-2570d as an altered plan prior to treatment authorization.
4.Change in Treatment plan by Fee Dentist. If circumstances necessitate a change in the treatment plan or if you disagree with the approved treatment plan, it will be necessary to contact the Chief of Dental Service at the issuing VA office (shown in Item 1) for approval of the change in the authorized services and fees prior to proceeding with the altered plan.
5.Spot check examinations. The VA routinely conducts a program of post-treatment clinical evaluations to assure satisfactory conclusion of the care authorized in the veteran's behalf. Pre-treatment examinations are also employed, as indicated, to assure consistency and appropriateness of planned treatment.
6.Time limitation for treatment. Treatment should be completed by the date shown in Item 28. If the patient does not respond for appointment, return the authorization to the issuing VA office (shown in Item 1). If, for good reason, an extension of time is required, please contact the same issuing office.
7.Restriction of Treatment. The VA outpatient dental care program operates under legal restrictions and, with few exceptions, only those conditions having been determined by VA to be "service-incurred" may be corrected at government expense.
8.Referral of Treatment.
a.If you find it necessary to refer any part of the authorized plan to another General Practitioner you may do so if the other dentist agrees to provide the care for the pre-authorized fees. The VA must be notified as to the identity of the other dentist and the specific services to be provided. Your original authorization must be amended by you to reflect your altered participation as well as the change to total fees which will be due to you.
b.If you find it necessary to refer any part of the authorized treatment to a Specialist you must first contact the Chief of Dental Service at the issuing VA office (shown in Item 1) prior to any referral (except in a true emergency). The VA must: (1) concur in the need for referral to a specialist; (2) confirm the specialty status of that individual; (3) negotiate with the specialist on appropriate fees for the specific services to be provided; or (4) determine if these services should be provided by VA staff.
9.Incomplete treatment. If for reasons beyond your control, you are unable to complete treatment as authorized, you should return the VA Form 10-2570d indicating the completed portions of treatment with an explanation of circumstances attached. If the patient has moved and has contacted you, please include the new address. Undelivered prostheses should be forwarded to the issuing VA office (shown in Item 1) along with your returned documents.
10.Questions concerning treatment or procedure. If any questions arise concerning dental care or procedures, contact the Chief of Dental Service at the issuing VA office (shown in Item 1). Clarification and/or concurrence will provide for proper procedure sequences and avoid undue problems.
11.Exclusion of dentists on active military duty. Dentists who are currently on active military duty and engaged in part-time private practice may not participate as fee dentists in the treatment of authorized veteran beneficiaries. The Comptroller General's decision 505, April 1, 1968 prohibits VA from making payments to members of the military service since, in their determination, it constitutes dual compensation of the dentist by the Federal Government. If dental treatment is provided under these circumstances, neither the VA or the veteran will be obligated for payment.
VA FORM |
|
|
MAR 2008 (R) 10-2570D |
DENTIST: NO PAYMENT WILL BE MADE UNLESS PRE-AUTHORIZED BY VA |
Instructions |
NOTE: If completing this form manually, please press firmly using a ballpoint pen.
OMB Number: 2900-0335
Estimated burden: 20 min.
DENTAL RECORD AUTHORIZATION AND
INVOICE FOR OUTPATIENT SERVICES
Paperwork Reduction Act: This data collection is in accordance with the clearance requirements of 5 CFR Part 1320. We may not conduct or sponsor, and you are not required to respond to, a collection of information unless it displays a valid OMB number. We anticipate that the time expended by all individuals who must complete this form will average 20 minutes. This includes the time it will take to read instructions, gather the necessary facts and fill out the form. This data is collected to authorize treatment, list the dental needs and serve as an invoice for treatment provided. Response is voluntary and failure to respond will have no impact on any benefits to which you may be entitled.
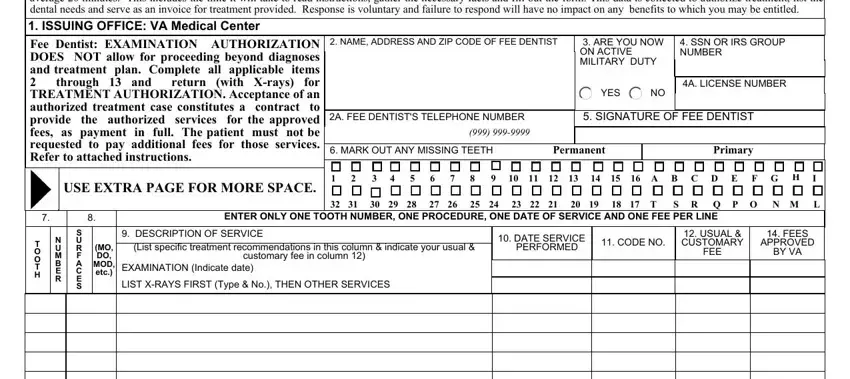
1. ISSUING OFFICE: VA MEDICAL CENTER
Fee Dentist: EXAMINATION |
AUTHORIZATION |
2. NAME, ADDRESS AND ZIP CODE OF FEE DENTIST |
|
|
3. ARE YOU NOW |
4. SSN OR IRS GROUP |
DOES |
NOT allow for proceeding beyond diagnoses |
|
|
|
|
|
|
|
ON ACTIVE |
|
NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MILITARY DUTY |
|
|
|
|
|
|
|
|
|
|
|
|
|
and treatment |
plan. Complete |
all applicable items |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
through |
13 |
and |
return |
(with X-rays) for |
|
|
|
|
|
|
|
|
|
|
4A. LICENSE NUMBER |
TREATMENT AUTHORIZATION. Acceptance of an |
|
|
|
|
|
|
|
|
YES |
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
authorized treatment case constitutes a contract to |
|
|
|
|
|
|
|
|
|
|
|
|
|
provide |
the |
authorized |
services for the approved |
2A. FEE DENTIST'S TELEPHONE NUMBER |
|
|
|
5. SIGNATURE OF FEE DENTIST |
|
fees, |
|
as |
payment in full. The patient must not be |
|
(999) 999-9999 |
|
|
|
|
|
|
|
|
|
requested to pay additional fees for those services. |
|
|
|
|
|
|
6. MARK OUT ANY MISSING TEETH |
Permanent |
|
Primary |
|
Refer to attached instructions. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 2 |
3 4 5 6 7 8 |
9 10 11 12 13 14 15 16 A B C D E F G H I |
|
|
|
|
|
|
|
|
|
|
|
|
USE EXTRA PAGE FOR MORE SPACE. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32 31 |
30 29 28 27 26 25 |
24 23 22 |
21 |
20 19 18 17 |
T |
S R Q P O |
N M L |
7. |
|
|
|
8. |
|
|
|
|
ENTER ONLY ONE TOOTH NUMBER, ONE PROCEDURE, ONE DATE OF SERVICE AND ONE FEE PER LINE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
N |
S |
|
|
|
9. DESCRIPTION OF SERVICE |
|
|
|
10. DATE SERVICE |
|
|
12. USUAL & |
|
14. FEES |
T |
U |
|
|
|
|
|
|
|
|
|
11. CODE NO. |
CUSTOMARY |
|
APPROVED |
U |
R |
(MO, |
(List specific treatment recommendations in this column & indicate your usual & |
|
PERFORMED |
|
|
O |
|
|
|
|
FEE |
|
BY VA |
M |
F |
DO, |
|
|
customary fee in column 12) |
|
|
|
|
|
|
|
|
|
|
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
A |
MOD, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
T |
EXAMINATION (Indicate date) |
|
|
|
|
|
|
|
|
|
|
|
|
|
E |
C |
ETC.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
H |
|
|
|
|
|
|
|
|
|
|
|
|
|
RE
SLIST X-RAYS FIRST (Type & No.), THEN OTHER SERVICES
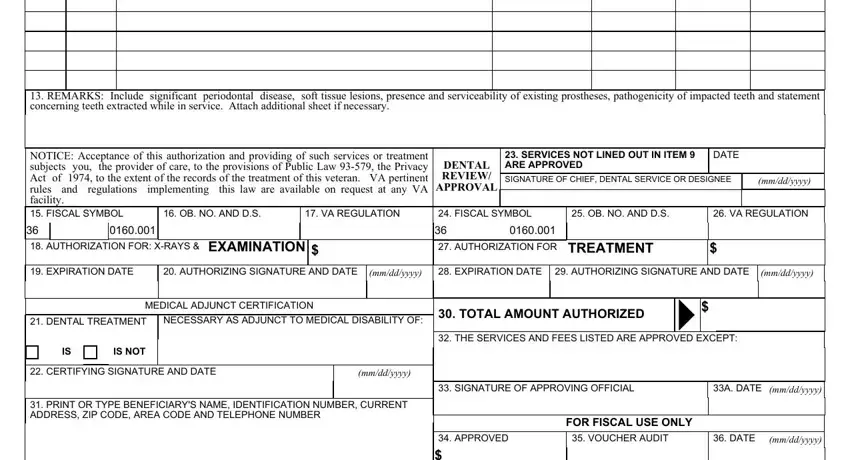
13.REMARKS: Include significant periodontal disease, soft tissue lesions, presence and serviceability of existing prostheses, pathogenicity of impacted teeth and statement concerning teeth extracted while in service. Attach additional sheet if necessary.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTICE: Acceptance of this authorization and providing of such services or treatment |
|
|
23. SERVICES NOT LINED OUT IN ITEM 9 |
DATE |
|
subjects |
you, the provider of care, to the provisions of Public Law 93-579, the Privacy |
DENTAL |
ARE APPROVED |
|
|
|
Act |
of |
1974, to the extent of the records of the treatment of this veteran. |
VA pertinent |
REVIEW/ |
SIGNATURE OF CHIEF, DENTAL SERVICE OR DESIGNEE |
|
(mm/dd/yyyy) |
rules |
and regulations |
implementing this law are available on request at any VA |
APPROVAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
facility. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. FISCAL SYMBOL |
|
16. OB. NO. AND D.S. |
17. VA REGULATION |
24. FISCAL SYMBOL |
25. OB. NO. AND D.S. |
26. VA REGULATION |
36 |
|
|
0160.001 |
|
|
|
|
36 |
|
0160.001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
18. AUTHORIZATION FOR: X-RAYS & EXAMINATION |
$ |
|
27. AUTHORIZATION FOR |
TREATMENT |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. EXPIRATION DATE |
|
20. AUTHORIZING SIGNATURE AND DATE |
(mm/dd/yyyy) |
28. EXPIRATION DATE |
29. AUTHORIZING SIGNATURE AND DATE |
(mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL ADJUNCT CERTIFICATION
21. DENTAL TREATMENT |
NECESSARY AS ADJUNCT TO MEDICAL DISABILITY OF: |
|
IS |
|
IS NOT |
|
|
|
|
|
|
|
|
|
|
|
|
22. CERTIFYING SIGNATURE AND DATE |
(mm/dd/yyyy) |
|
|
|
|
|
|
31.PRINT OR TYPE BENEFICIARY'S NAME, IDENTIFICATION NUMBER, CURRENT ADDRESS, ZIP CODE, AREA CODE AND TELEPHONE NUMBER
30. TOTAL AMOUNT AUTHORIZED |
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
32. THE SERVICES AND FEES LISTED ARE APPROVED EXCEPT: |
|
33. SIGNATURE OF APPROVING OFFICIAL |
|
33A. DATE |
|
|
(mm/dd/yyyy) |
|
|
|
|
FOR FISCAL USE ONLY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
34. APPROVED |
35. VOUCHER AUDIT |
|
36. DATE |
(mm/dd/yyyy) |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
STA. # |
|
PAT. # |
T/C & S/C |
|
INITIALS |
|
DATE |
(mm/dd/yyyy) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VA FORM |
10-2570D |
DENTIST: NO PAYMENT WILL BE MADE UNLESS PRE-AUTHORIZED BY VA |
MAR 2008 (R) |