Are you looking for information on VA Form 24-5281? If so, you've come to the right place. In this blog post, we'll provide a detailed overview of what VA form 24-5281 is used for and how it can help veterans or their survivors make claims for disability compensation or death benefits from the Department of Veterans Affairs (VA). We'll also share some tips on how to successfully complete the form and answer any frequently asked questions about it. Read on to learn more about VA Form 24-5281!
| Question | Answer |
|---|---|
| Form Name | Va Form 24 5281 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 24 5281 omb veap refund form |
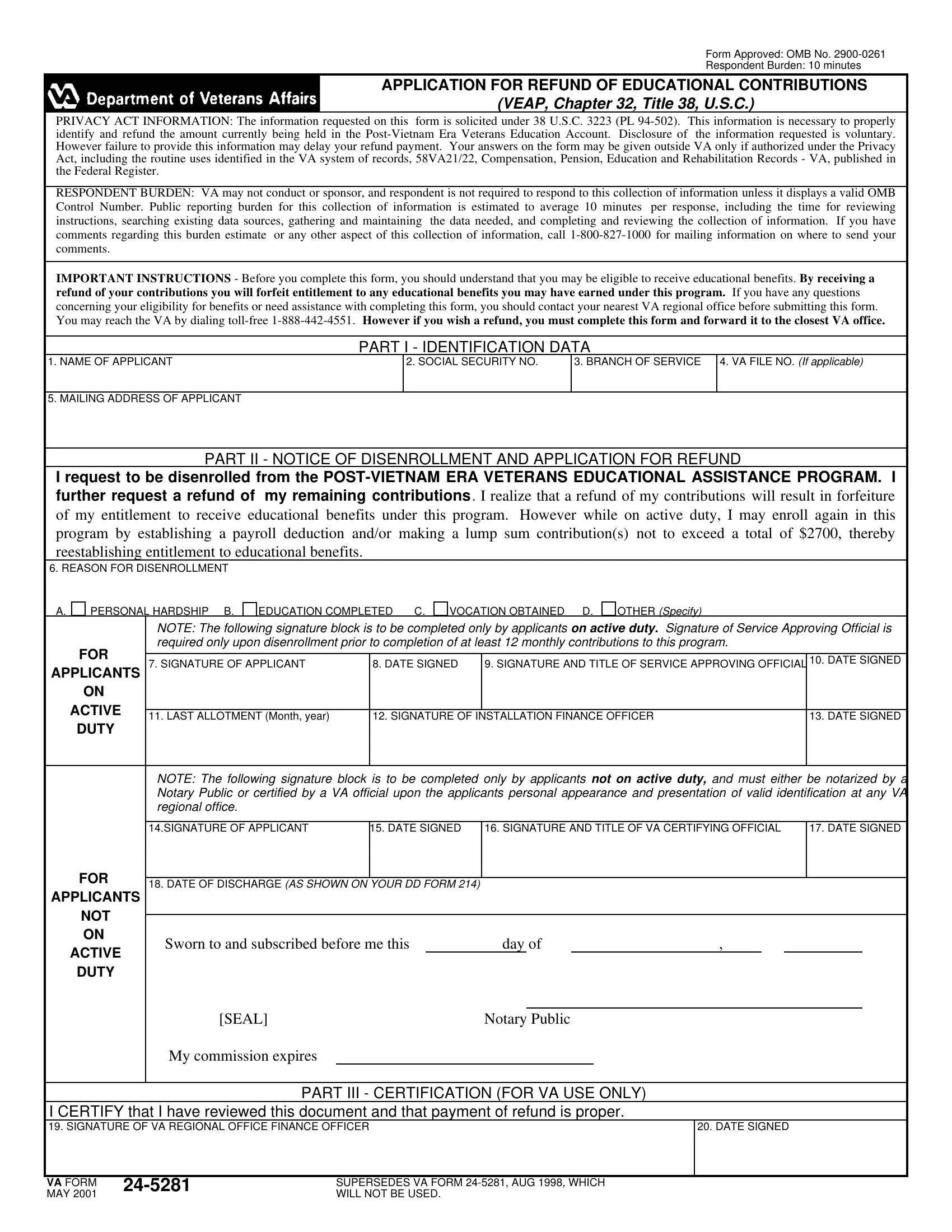
Form Approved: OMB No.
Respondent Burden: 10 minutes
APPLICATION FOR REFUND OF EDUCATIONAL CONTRIBUTIONS
(VEAP, Chapter 32, Title 38, U.S.C.)
PRIVACY ACT INFORMATION: The information requested on this form is solicited under 38 U.S.C. 3223 (PL
RESPONDENT BURDEN: VA may not conduct or sponsor, and respondent is not required to respond to this collection of information unless it displays a valid OMB Control Number. Public reporting burden for this collection of information is estimated to average 10 minutes per response, including the time for reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. If you have comments regarding this burden estimate or any other aspect of this collection of information, call
IMPORTANT INSTRUCTIONS - Before you complete this form, you should understand that you may be eligible to receive educational benefits. By receiving a refund of your contributions you will forfeit entitlement to any educational benefits you may have earned under this program. If you have any questions
concerning your eligibility for benefits or need assistance with completing this form, you should contact your nearest VA regional office before submitting this form.
You may reach the VA by dialing
PART I - IDENTIFICATION DATA
1. NAME OF APPLICANT
2. SOCIAL SECURITY NO.
3. BRANCH OF SERVICE
4.VA FILE NO. (If applicable)
5. MAILING ADDRESS OF APPLICANT
PART II - NOTICE OF DISENROLLMENT AND APPLICATION FOR REFUND
I request to be disenrolled from the
6. REASON FOR DISENROLLMENT
A.
PERSONAL HARDSHIP B.
EDUCATION COMPLETED C.
VOCATION OBTAINED D.
OTHER (Specify)
NOTE: The following signature block is to be completed only by applicants on active duty. Signature of Service Approving Official is required only upon disenrollment prior to completion of at least 12 monthly contributions to this program.
FOR |
|
|
|
|
|
7. SIGNATURE OF APPLICANT |
8. DATE SIGNED |
9. SIGNATURE AND TITLE OF SERVICE APPROVING OFFICIAL |
10. DATE SIGNED |
||
APPLICANTS |
|||||
|
|
|
|
||
ON |
|
|
|
|
|
ACTIVE |
|
|
|
|
|
11. LAST ALLOTMENT (Month, year) |
12. SIGNATURE OF INSTALLATION FINANCE OFFICER |
13. DATE SIGNED |
|||
|
|||||
DUTY |
|
|
|
|
|
|
|
|
|
|
|
NOTE: The following signature block is to be completed only by applicants not on active duty, and must either be notarized by a Notary Public or certified by a VA official upon the applicants personal appearance and presentation of valid identification at any VA regional office.
14.SIGNATURE OF APPLICANT |
15. DATE SIGNED |
16. SIGNATURE AND TITLE OF VA CERTIFYING OFFICIAL |
17. DATE SIGNED |
FOR |
|
|
|
|
|
|
|
|
18. DATE OF DISCHARGE (AS SHOWN ON YOUR DD FORM 214) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
APPLICANTS |
|
|
|
|
|
|
|
|
NOT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ON |
Sworn to and subscribed before me this |
day of |
, |
|
|
|
||
ACTIVE |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
DUTY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[SEAL] |
Notary Public |
|
|
|
|
||
My commission expires
PART III - CERTIFICATION (FOR VA USE ONLY)
I CERTIFY that I have reviewed this document and that payment of refund is proper.
19. SIGNATURE OF VA REGIONAL OFFICE FINANCE OFFICER
20. DATE SIGNED
VA FORM |
SUPERSEDES VA FORM |
|
|
||
MAY 2001 |
|
WILL NOT BE USED. |