
Whenever you want to fill out va form 3949, you won't have to download any software - simply try using our PDF tool. To keep our tool on the cutting edge of efficiency, we strive to integrate user-driven capabilities and enhancements on a regular basis. We are routinely looking for suggestions - join us in reshaping how we work with PDF documents. To get the process started, go through these easy steps:
Step 1: Simply hit the "Get Form Button" in the top section of this page to see our pdf file editor. This way, you will find all that is necessary to work with your file.
Step 2: After you launch the PDF editor, there'll be the form prepared to be filled out. Other than filling out different blanks, you may also perform several other things with the form, specifically adding your own words, changing the initial text, adding illustrations or photos, putting your signature on the document, and more.
To be able to finalize this form, make certain you enter the right details in each and every blank:
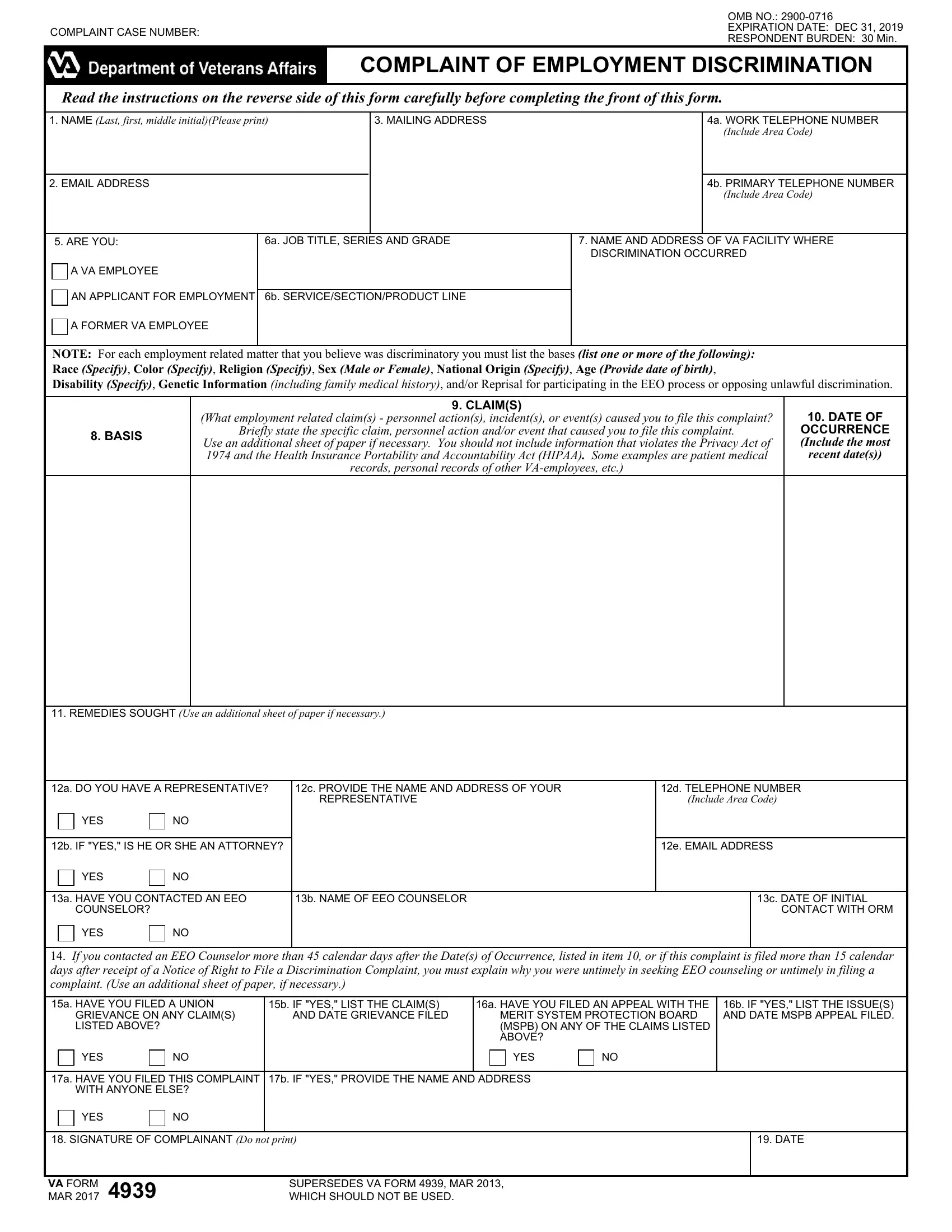
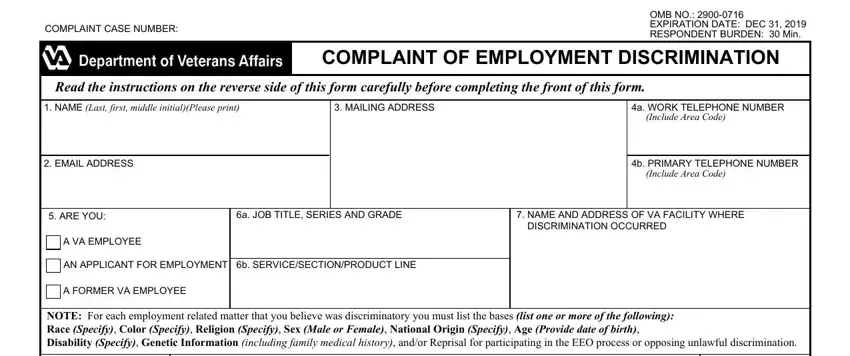
1. It is crucial to complete the va form 3949 correctly, so pay close attention while filling in the segments containing all of these blank fields:
2. After the previous part is finished, it's time to insert the essential specifics in Use an additional sheet of paper, records personal records of other, recent dates, REMEDIES SOUGHT Use an additional, a DO YOU HAVE A REPRESENTATIVE, c PROVIDE THE NAME AND ADDRESS OF, d TELEPHONE NUMBER Include Area, YES, b IF YES IS HE OR SHE AN ATTORNEY, e EMAIL ADDRESS, YES, a HAVE YOU CONTACTED AN EEO, b NAME OF EEO COUNSELOR, c DATE OF INITIAL CONTACT WITH ORM, and YES so you're able to move on further.
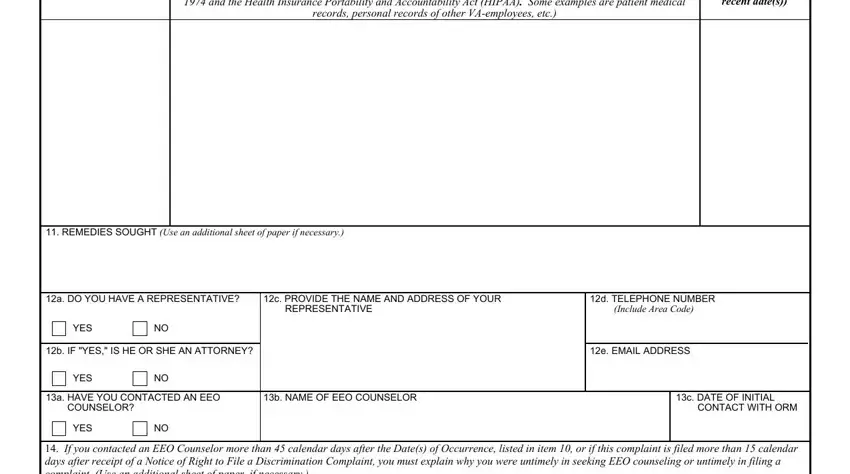
People generally make some mistakes when completing d TELEPHONE NUMBER Include Area in this section. Don't forget to read again what you enter here.
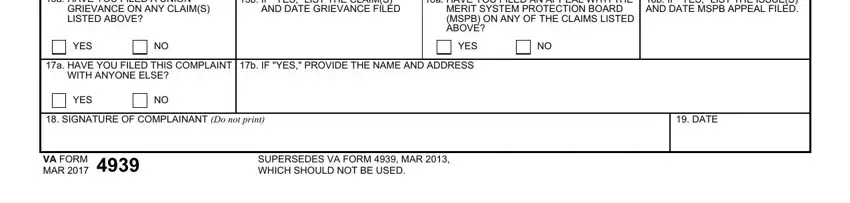
3. This subsequent part should also be relatively simple, a HAVE YOU FILED A UNION GRIEVANCE, b IF YES LIST THE CLAIMS AND DATE, a HAVE YOU FILED AN APPEAL WITH, b IF YES LIST THE ISSUES AND DATE, YES, YES, a HAVE YOU FILED THIS COMPLAINT, b IF YES PROVIDE THE NAME AND, YES, SIGNATURE OF COMPLAINANT Do not, DATE, VA FORM, MAR, and SUPERSEDES VA FORM MAR WHICH - each one of these empty fields must be filled in here.
Step 3: When you have looked over the information in the document, simply click "Done" to conclude your document creation. Grab your va form 3949 as soon as you join for a 7-day free trial. Readily view the pdf document within your FormsPal account page, with any edits and adjustments automatically synced! Here at FormsPal.com, we do our utmost to make sure that all your information is kept private.