
You could prepare vermont accident report today effectively with our PDFinity® online tool. In order to make our tool better and more convenient to utilize, we continuously work on new features, with our users' suggestions in mind. All it requires is several basic steps:
Step 1: First of all, access the editor by clicking the "Get Form Button" at the top of this site.
Step 2: With this handy PDF tool, you may do more than just fill in forms. Try each of the functions and make your docs look great with custom textual content put in, or optimize the file's original content to perfection - all that comes with the capability to incorporate your own pictures and sign the file off.
So as to fill out this form, be sure you enter the information you need in each blank:
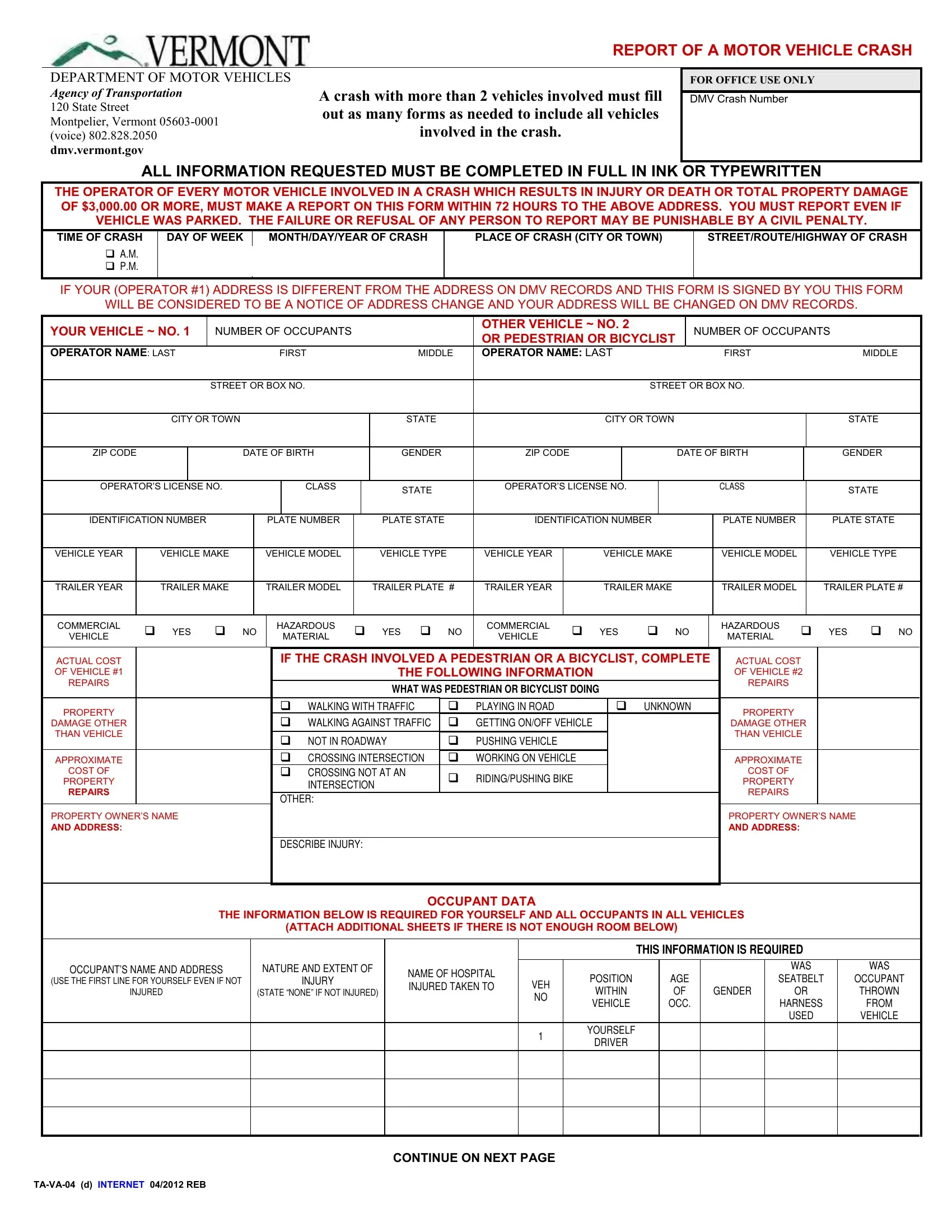
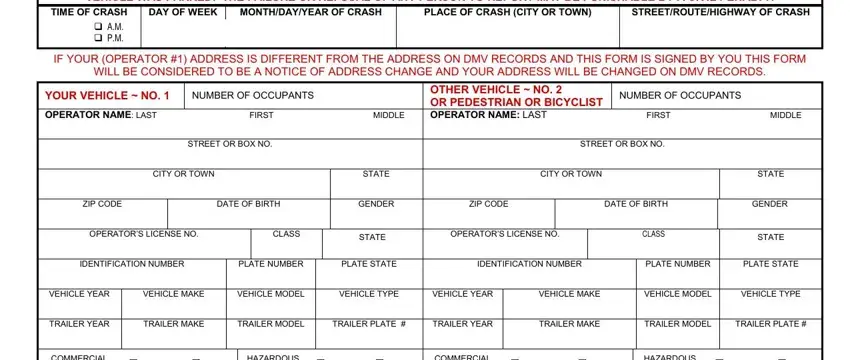
1. The vermont accident report today involves particular information to be entered. Be sure the next blanks are filled out:
2. The next stage would be to submit the next few blank fields: COMMERCIAL, VEHICLE, cid, YES cid NO, HAZARDOUS, MATERIAL, cid, YES cid NO, COMMERCIAL, VEHICLE, cid, YES, cid NO, HAZARDOUS, and MATERIAL.
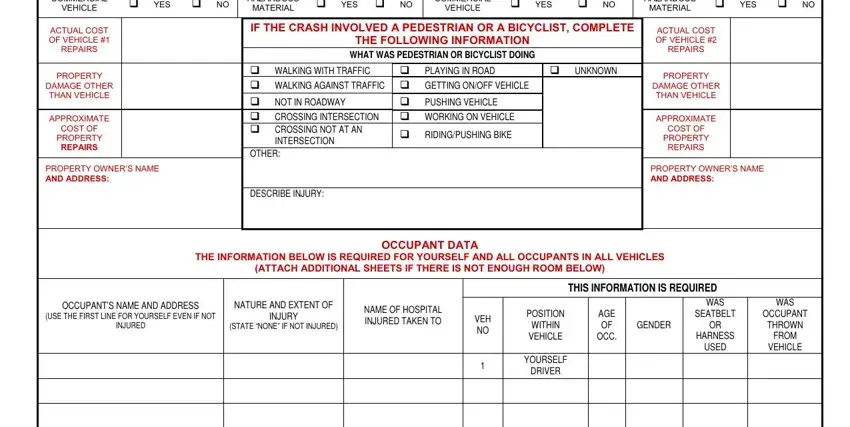
People generally make mistakes when completing VEHICLE in this part. Remember to go over everything you type in here.
3. The next part is easy - fill in all of the fields in TAVA d INTERNET REB, and CONTINUE ON NEXT PAGE to conclude this segment.

4. You're ready to complete the next portion! Here you will get these DESCRIBE IN YOUR OWN WORDS WHAT form blanks to fill in.
5. Lastly, the following final subsection is precisely what you will have to finish prior to closing the document. The blanks here include the following: WAS THIS CRASH INVESTIGATED BY AN, Yes, cid, IF YES GIVE NAME OF OFFICER, OFFICERS DEPARTMENT, WERE YOU DRIVING A COMMERCIAL, cid Yes, cid No, WAS THE VEHICLE TRANSPORTING, cid No, IF YES GIVE NAME OF MATERIAL, OPERATOR SIGN HERE cid, DATE OF REPORT, and CONTINUE ON NEXT PAGE.
Step 3: Right after proofreading your entries, press "Done" and you are done and dusted! Get hold of your vermont accident report today as soon as you subscribe to a free trial. Easily gain access to the pdf form from your FormsPal account page, together with any edits and adjustments being automatically saved! At FormsPal, we strive to make certain that all of your details are stored protected.