
vt rn renewal can be filled out online with ease. Just make use of FormsPal PDF tool to complete the job in a timely fashion. Our team is devoted to providing you with the ideal experience with our editor by constantly presenting new functions and upgrades. Our tool has become a lot more user-friendly as the result of the newest updates! Now, filling out documents is a lot easier and faster than ever before. To start your journey, take these basic steps:
Step 1: Access the PDF doc in our editor by clicking on the "Get Form Button" in the top area of this webpage.
Step 2: Using this state-of-the-art PDF file editor, it's possible to accomplish more than just fill out blank fields. Edit away and make your forms appear faultless with custom textual content added in, or optimize the file's original input to perfection - all comes with the capability to add your own pictures and sign it off.
This PDF form will require specific details to be filled out, therefore you must take the time to fill in precisely what is requested:
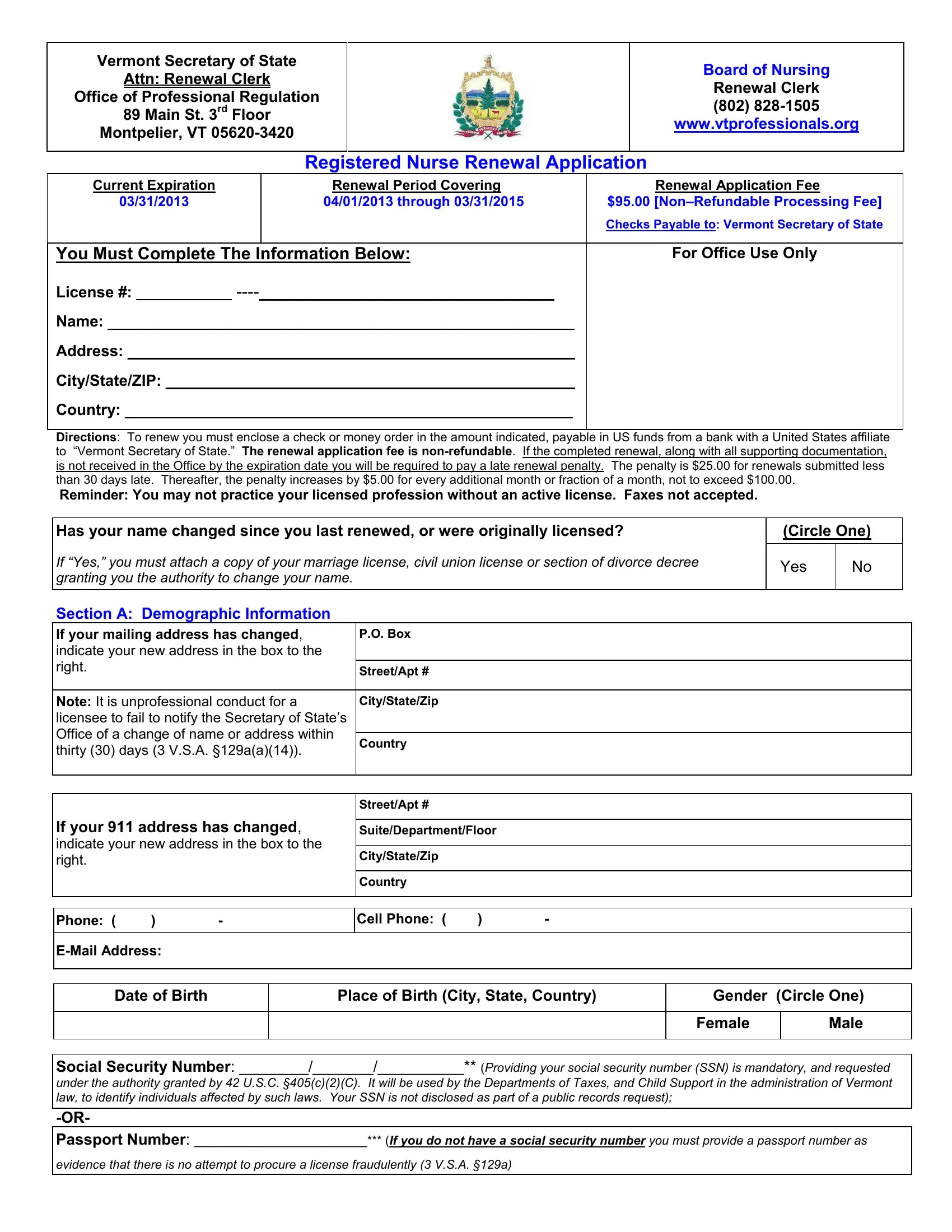
1. The vt rn renewal involves particular information to be entered. Be sure the subsequent blank fields are finalized:
2. After this array of blanks is completed, proceed to type in the applicable information in all these: Directions To renew you must, PO Box, StreetApt, Note It is unprofessional conduct, CityStateZip, Country, If your address has changed, StreetApt, SuiteDepartmentFloor, CityStateZip, Country, Phone, Cell Phone, EMail Address, and Date of Birth.
3. The following segment is generally rather easy, Social Security Number Providing, and evidence that there is no attempt - all of these form fields will have to be filled out here.

It's very easy to make a mistake when completing the Social Security Number Providing, so make sure that you take another look before you decide to finalize the form.
4. Filling out Child Support Orders VSA c As of, Not Applicable I am not subject, I am in good standing, I am in compliance with a payment, I am NOT in good standing, TAXES, Tax Compliance VSA b As of the, Not Applicable I have never lived, I am in good standing, I am in compliance with a payment, I am NOT in good standing, and DISTRICT COURT FINES JUDICIAL is crucial in the fourth step - make sure to don't hurry and be mindful with each and every blank!
5. As you reach the completion of the form, you'll find several more points to undertake. Particularly, Unpaid Judgments VSA b and c As, Not Applicable I do not have any, I am in good standing with the, I am NOT in good standing, and Good standing is defined in the must be done.
Step 3: Before moving on, it's a good idea to ensure that blanks were filled out as intended. As soon as you believe it's all fine, click on “Done." Make a free trial plan with us and get direct access to vt rn renewal - with all transformations preserved and accessible inside your personal cabinet. FormsPal guarantees your information privacy by having a protected system that never saves or shares any personal data typed in. Be confident knowing your docs are kept safe any time you use our tools!