

It is possible to complete epi 1 easily with the help of our PDFinity® editor. Our tool is constantly evolving to provide the best user experience attainable, and that's thanks to our resolve for constant development and listening closely to comments from users. This is what you'll want to do to get started:
Step 1: Press the orange "Get Form" button above. It's going to open our pdf editor so that you can begin completing your form.
Step 2: After you open the tool, you will notice the document all set to be completed. Besides filling in various fields, you could also perform other things with the Document, including writing custom textual content, changing the initial textual content, inserting graphics, signing the PDF, and much more.
It will be simple to finish the pdf using out detailed tutorial! This is what you have to do:
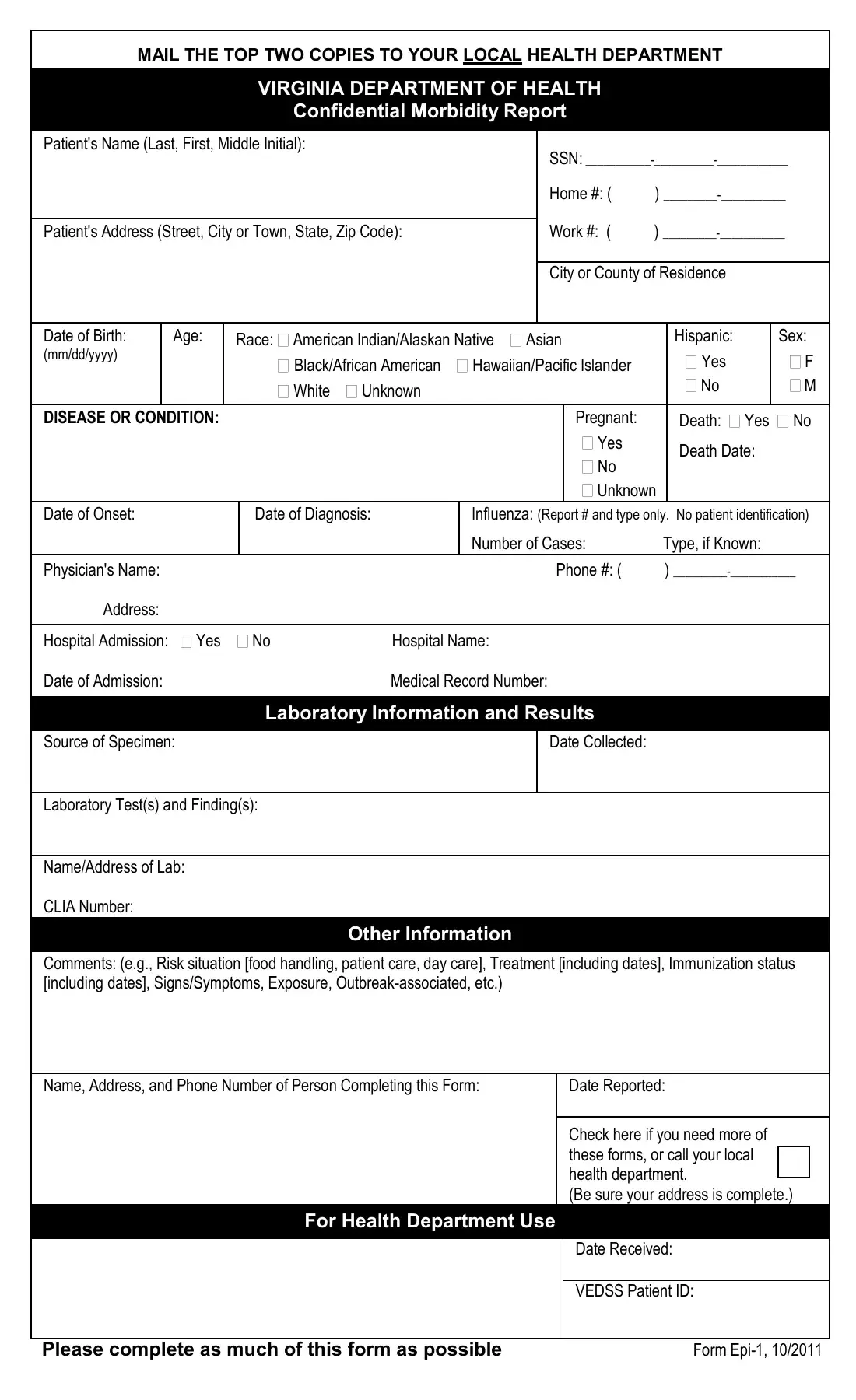
1. Begin filling out the epi 1 with a group of major fields. Collect all the information you need and ensure absolutely nothing is left out!
Step 3: Once you have reviewed the details in the file's blank fields, press "Done" to conclude your document creation. Right after setting up afree trial account with us, it will be possible to download epi 1 or send it through email without delay. The file will also be readily available through your personal account menu with your each and every change. We do not sell or share any details that you enter while dealing with forms at our site.