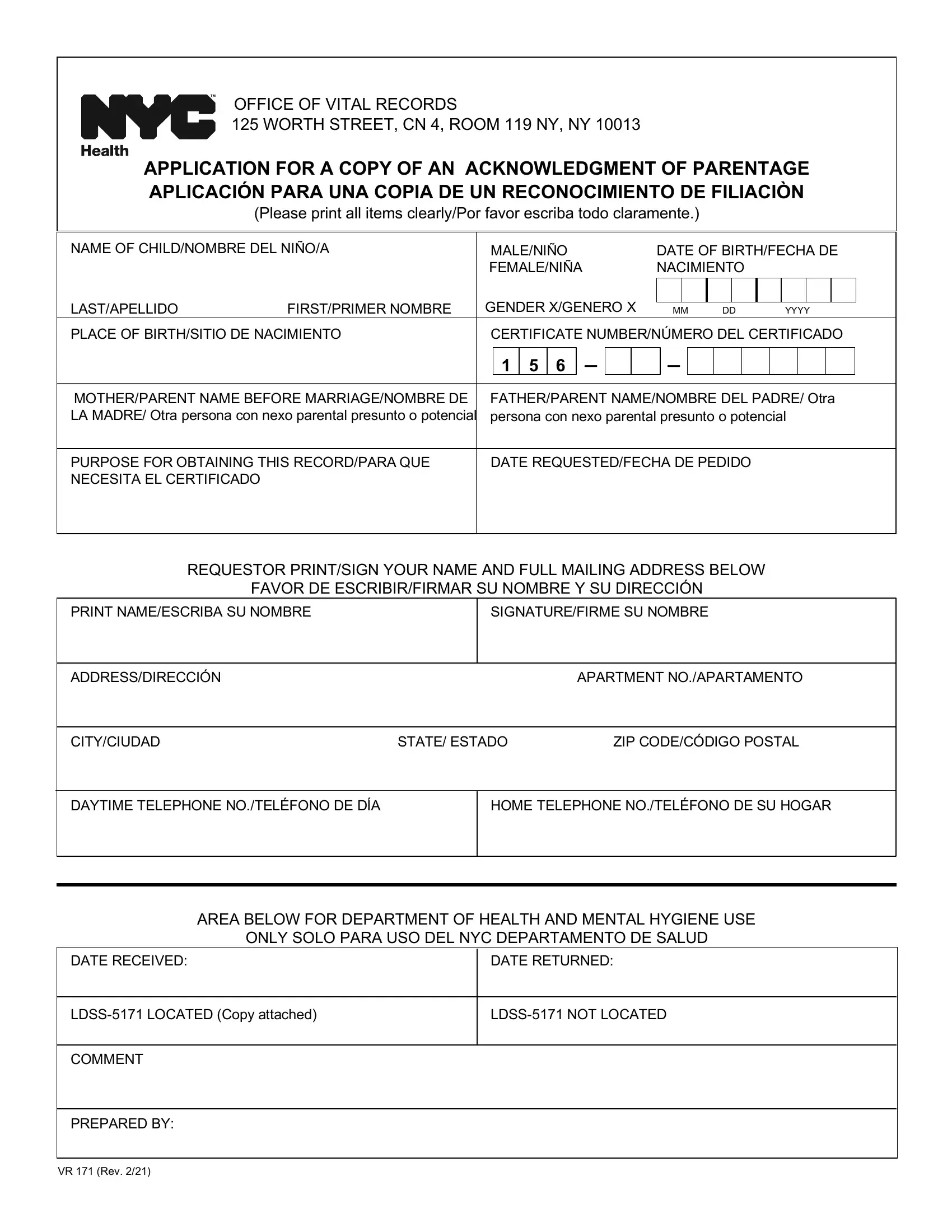
In the complex panorama of administrative procedures, the VR 171 form serves a crucial function, particularly for families and individuals navigating the nuances of legal parentage in New York. Located within the labyrinthine corridors of the Office of Vital Records at 125 Worth Street, this document facilitates the acquisition of an official Acknowledgment of Parentage, marking a pivotal step in affirming the legal relationship between a parent and a child. Its significance extends beyond the mere formal recognition of a biological connection, impacting a range of legal rights, responsibilities, and access to vital records. The form requires detailed information, including the child's name, date of birth, place of birth, and certificate number, alongside the parent or guardian's details and their reason for requesting the record. The process underscores the importance of clarity and accuracy, from the stipulation that all items be printed clearly to the necessity of including a current photo identification with the application. Interestingly, the form highlights an accommodating stance towards various family structures by providing space for the names of parents or other potential parental figures, reflecting evolving social norms and legal recognitions. Furthermore, it is noteworthy that obtaining this acknowledgment incurs no fee, removing a potential barrier to formalizing parent-child relationships. The instructions at the conclusion of the VR 171 form underscore the exclusivity of the entitlement to order the record to the persons listed on the existing Acknowledgment of Parentage (AOP), ensuring a layer of privacy and protection to the involved parties. This document, thereby, encapsulates a blend of bureaucratic procedure and the acknowledgment of changing familial dynamics, positioned within the broader context of health and legal systems at the city level.
| Question | Answer |
|---|---|
| Form Name | Vr 171 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | acknowledgement of paternity form nyc, vr 171, how to get a copy of acknowledgement of paternity in nyc, paternity form ny |
OFFICE OF VITAL RECORDS
125 WORTH STREET, CN 4, ROOM 119 NY, NY 10013
APPLICATION FOR A COPY OF AN ACKNOWLEDGMENT OF PARENTAGE APLICACIÓN PARA UNA COPIA DE UN RECONOCIMIENTO DE FILIACIÒN
(Please print all items clearly/Por favor escriba todo claramente.)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME OF CHILD/NOMBRE DEL NIÑO/A |
|
|
|
MALE/NIÑO |
|
|
DATE OF BIRTH/FECHA DE |
|
||||||||||||||||||||
|
|
|
|
|
|
FEMALE/NIÑA |
|
|
NACIMIENTO |
|
|
|
|
|
|
|
|||||||||||||
|
LAST/APELLIDO |
FIRST/PRIMER NOMBRE |
|
|
GENDER X/GENERO X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
MM |
DD |
YYYY |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BIRTH/SITIO DE NACIMIENTO |
|
|
|
CERTIFICATE NUMBER/NÚMERO DEL CERTIFICADO |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
1 |
5 |
6 |
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTHER/PARENT NAME BEFORE MARRIAGE/NOMBRE DE |
|
|
|
FATHER/PARENT NAME/NOMBRE DEL PADRE/ Otra |
|
|||||||||||||||||||||||
|
LA MADRE/ Otra persona con nexo parental presunto o potencial |
|
|
|
persona con nexo parental presunto o potencial |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PURPOSE FOR OBTAINING THIS RECORD/PARA QUE |
|
|
|
DATE REQUESTED/FECHA DE PEDIDO |
|
|
|
|
|
|
|
|||||||||||||||||
|
NECESITA EL CERTIFICADO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REQUESTOR PRINT/SIGN YOUR NAME AND FULL MAILING ADDRESS BELOW |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
FAVOR DE ESCRIBIR/FIRMAR SU NOMBRE Y SU DIRECCIÓN |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
PRINT NAME/ESCRIBA SU NOMBRE |
|
|
|
SIGNATURE/FIRME SU NOMBRE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
ADDRESS/DIRECCIÓN |
|
|
|
|
|
|
|
APARTMENT NO./APARTAMENTO |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
CITY/CIUDAD |
STATE/ ESTADO |
ZIP CODE/CÓDIGO POSTAL |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAYTIME TELEPHONE NO./TELÉFONO DE DÍA |
|
|
|
HOME TELEPHONE NO./TELÉFONO DE SU HOGAR |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AREA BELOW FOR DEPARTMENT OF HEALTH AND MENTAL HYGIENE USE
ONLY SOLO PARA USO DEL NYC DEPARTAMENTO DE SALUD
|
DATE RECEIVED: |
|
|
DATE RETURNED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREPARED BY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VR 171 (Rev. 2/21)
Instructions:
•Only the person(s) listed on the existing AOP are entitled to order the record.
•Please include a copy of your current photo Identification with this application.
•There is no fee to order an existing AOP.
•Mail the completed application to:
New York City DOHMH
Office of Vital Records Services
125 Worth Street, CN 4, Room 119
NY, NY 10013