Are you looking to apply for a visa and are having trouble understanding the paperwork? Trying to figure out how to fill out Form VR 171 can be incredibly confusing and frustrating, particularly when it seems like there is so much to consider. We understand that applying for visas can seem daunting - but don't worry! In this blog post we will be breaking down each part of the Vr 171 Form application process in an easy-to-understand way so you have all of the information you need before getting started.
| Question | Answer |
|---|---|
| Form Name | Vr 171 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | acknowledgement of paternity form nyc, vr 171, how to get a copy of acknowledgement of paternity in nyc, paternity form ny |
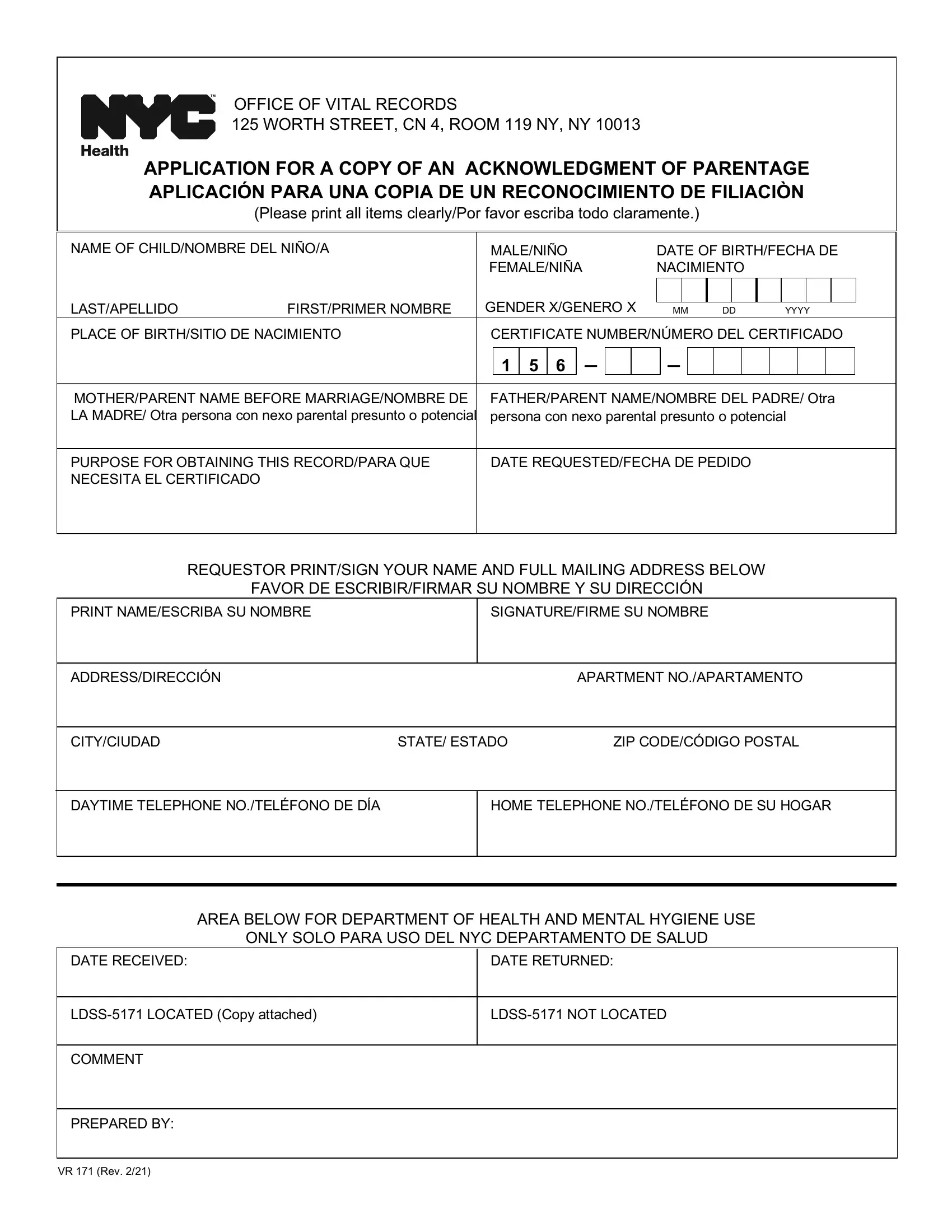
OFFICE OF VITAL RECORDS
125 WORTH STREET, CN 4, ROOM 119 NY, NY 10013
APPLICATION FOR A COPY OF AN ACKNOWLEDGMENT OF PARENTAGE APLICACIÓN PARA UNA COPIA DE UN RECONOCIMIENTO DE FILIACIÒN
(Please print all items clearly/Por favor escriba todo claramente.)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME OF CHILD/NOMBRE DEL NIÑO/A |
|
|
|
MALE/NIÑO |
|
|
DATE OF BIRTH/FECHA DE |
|
||||||||||||||||||||
|
|
|
|
|
|
FEMALE/NIÑA |
|
|
NACIMIENTO |
|
|
|
|
|
|
|
|||||||||||||
|
LAST/APELLIDO |
FIRST/PRIMER NOMBRE |
|
|
GENDER X/GENERO X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
MM |
DD |
YYYY |
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLACE OF BIRTH/SITIO DE NACIMIENTO |
|
|
|
CERTIFICATE NUMBER/NÚMERO DEL CERTIFICADO |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
1 |
5 |
6 |
– |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MOTHER/PARENT NAME BEFORE MARRIAGE/NOMBRE DE |
|
|
|
FATHER/PARENT NAME/NOMBRE DEL PADRE/ Otra |
|
|||||||||||||||||||||||
|
LA MADRE/ Otra persona con nexo parental presunto o potencial |
|
|
|
persona con nexo parental presunto o potencial |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PURPOSE FOR OBTAINING THIS RECORD/PARA QUE |
|
|
|
DATE REQUESTED/FECHA DE PEDIDO |
|
|
|
|
|
|
|
|||||||||||||||||
|
NECESITA EL CERTIFICADO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REQUESTOR PRINT/SIGN YOUR NAME AND FULL MAILING ADDRESS BELOW |
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
FAVOR DE ESCRIBIR/FIRMAR SU NOMBRE Y SU DIRECCIÓN |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
PRINT NAME/ESCRIBA SU NOMBRE |
|
|
|
SIGNATURE/FIRME SU NOMBRE |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
ADDRESS/DIRECCIÓN |
|
|
|
|
|
|
|
APARTMENT NO./APARTAMENTO |
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
CITY/CIUDAD |
STATE/ ESTADO |
ZIP CODE/CÓDIGO POSTAL |
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DAYTIME TELEPHONE NO./TELÉFONO DE DÍA |
|
|
|
HOME TELEPHONE NO./TELÉFONO DE SU HOGAR |
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AREA BELOW FOR DEPARTMENT OF HEALTH AND MENTAL HYGIENE USE
ONLY SOLO PARA USO DEL NYC DEPARTAMENTO DE SALUD
|
DATE RECEIVED: |
|
|
DATE RETURNED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMMENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PREPARED BY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VR 171 (Rev. 2/21)
Instructions:
•Only the person(s) listed on the existing AOP are entitled to order the record.
•Please include a copy of your current photo Identification with this application.
•There is no fee to order an existing AOP.
•Mail the completed application to:
New York City DOHMH
Office of Vital Records Services
125 Worth Street, CN 4, Room 119
NY, NY 10013