
When working in the online editor for PDFs by FormsPal, it is easy to fill out or alter washington application food here. We at FormsPal are devoted to providing you the best possible experience with our tool by constantly adding new functions and upgrades. Our editor is now much more intuitive as the result of the most recent updates! Now, working with PDF forms is a lot easier and faster than ever. To start your journey, take these easy steps:
Step 1: First, access the pdf tool by pressing the "Get Form Button" at the top of this page.
Step 2: With our advanced PDF file editor, you could accomplish more than merely fill in blank fields. Edit away and make your documents seem faultless with customized textual content added, or optimize the original input to perfection - all comes with the capability to add your own graphics and sign it off.
Pay close attention when completing this document. Make sure that each blank is done properly.
1. Complete the washington application food with a selection of necessary blank fields. Gather all of the information you need and ensure there is nothing left out!
2. When this part is completed, proceed to enter the applicable details in these - LAST, YOU, Myself, CHECK IF YOU WANT BENEFITS FOR, SECURITY NUMBER, CHECK IF US CITIZEN, BELOW, TRIBE NAME For American Indians, Nativ es, My ethnic background is Hispanic, Yes, and Race and Ethnic background.
3. This subsequent segment is typically rather uncomplicated, APPLICANTS NAME, SOCIAL SECURITY NUMBER, CLIENT IDENTIFICATION NUMBER, I General Information, In the past days I received cash, No Who, No Who, Yes, Yes, High School, Yes, a High School Equivalency Program, Trade School Who, College Yes, and No Who - each one of these fields has to be filled out here.
4. To go forward, this fourth form section involves typing in a couple of blanks. Examples of these are I or someone in my home was, September, Yes, Yes, Yes II Resources Attach Proof For, No b A boarder, Yes, A resource is anything you own or, CDs Money market account Bonds, Trusts IRA k Homes Land or, Buildings, RESOURCE, WHO OWNS, LOCATION, and VALUE, which you'll find vital to continuing with this process.
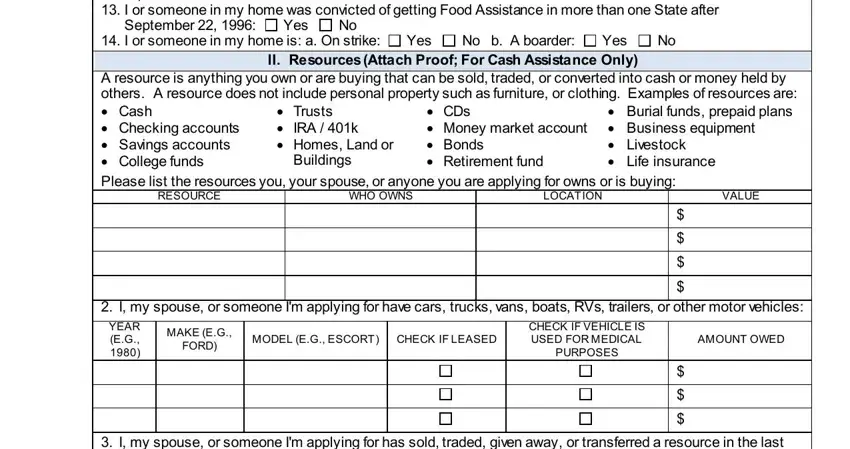
You can potentially make an error when completing the CDs Money market account Bonds, hence ensure that you take a second look before you decide to submit it.
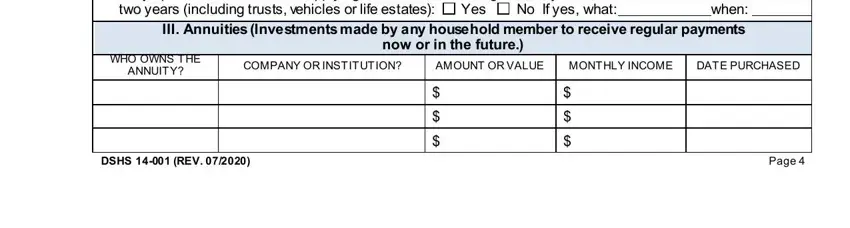
5. The very last section to submit this PDF form is pivotal. Be sure you fill in the required blanks, such as I my spouse or someone Im, two years including trusts, No If yes what, Yes, III Annuities Investments made by, now or in the future, WHO OWNS THE, ANNUITY, COMPANY OR INSTITUTION, AMOUNT OR VALUE, MONTHLY INCOME, DATE PURCHASED, DSHS REV, and Page, prior to finalizing. Failing to do so could lead to an incomplete and possibly nonvalid paper!
Step 3: Prior to finishing the document, check that all form fields were filled out the right way. Once you confirm that it is good, press “Done." Get hold of your washington application food the instant you sign up for a 7-day free trial. Easily gain access to the pdf inside your FormsPal account page, along with any modifications and adjustments automatically preserved! FormsPal guarantees secure form tools devoid of data record-keeping or sharing. Rest assured that your details are safe here!