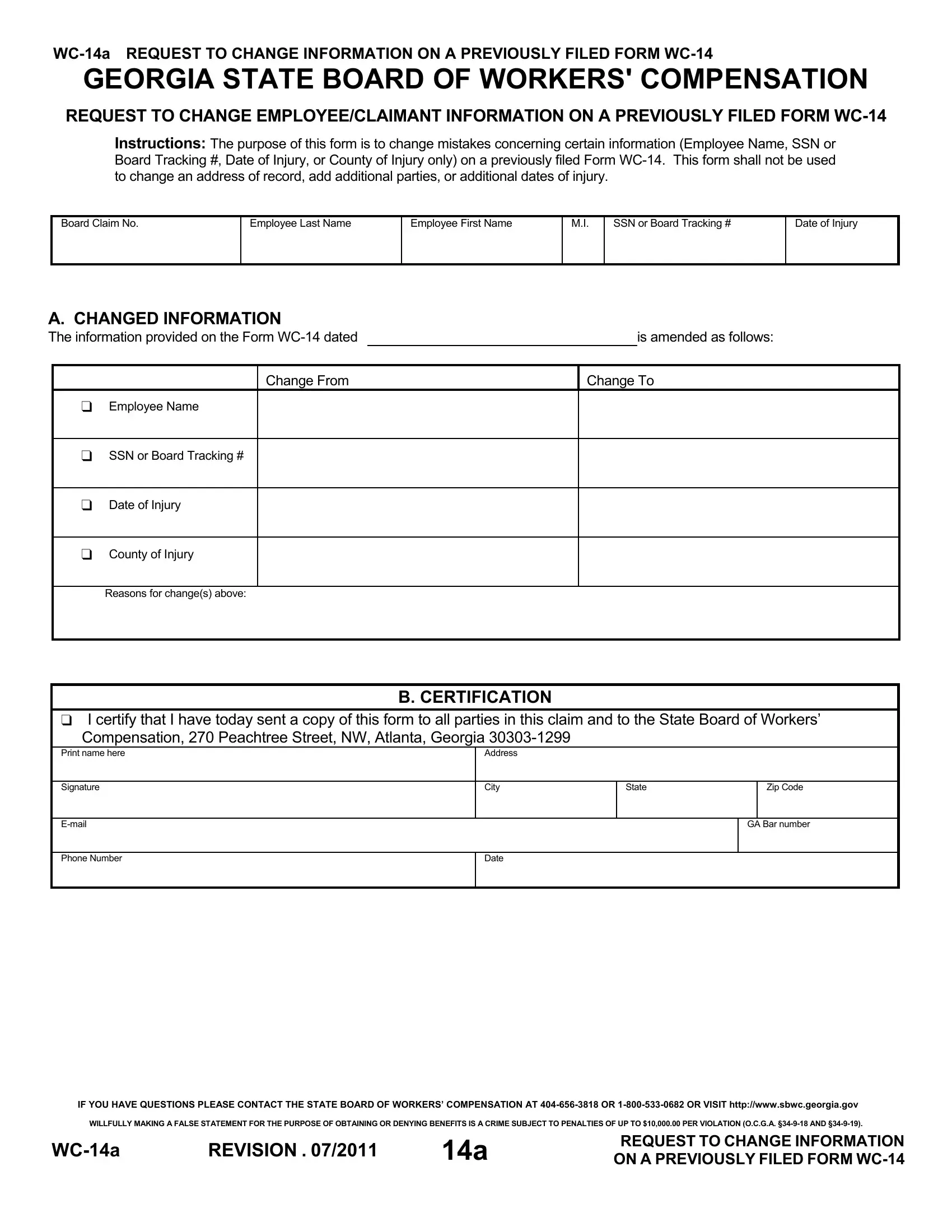
Understanding the nuances of workplace injury claims in Georgia involves familiarizing oneself with various forms and procedures, among which, the WC-14a form holds a critical place. This particular document is essentially used to correct or update specific pieces of information previously submitted on Form WC-14, the initial claim form for workers' compensation. It is specifically designed to address errors or changes needing to be made concerning the employee or claimant's name, Social Security Number or Board Tracking Number, the date of the injury, and the county where the injury occurred. Notably, it is not intended for use in changing addresses, adding parties to the claim, or listing additional injury dates, underscoring its focused purpose. Completing and submitting this form correctly is a key step in ensuring that the claim process proceeds without unnecessary delays or complications, particularly for rectifying essential personal and incident details. Moreover, it mandates certification and notification to all involved parties, emphasizing the form’s role in maintaining transparency and accountability throughout the workers' compensation claim process. This process also serves as a reminder of the severe legal consequences for providing false information in an attempt to manipulate benefit outcomes. As such, the WC-14a form is a vital tool for both employees and employers in the meticulous journey of workers' compensation claims in Georgia.
| Question | Answer |
|---|---|
| Form Name | Form Wc 14A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wc014a wc 14 form |
GEORGIA STATE BOARD OF WORKERS' COMPENSATION
REQUEST TO CHANGE EMPLOYEE/CLAIMANT INFORMATION ON A PREVIOUSLY FILED FORM
Instructions: The purpose of this form is to change mistakes concerning certain information (Employee Name, SSN or Board Tracking #, Date of Injury, or County of Injury only) on a previously filed Form
Board Claim No.
Employee Last Name
Employee First Name
M.I.
SSN or Board Tracking #
Date of Injury
A. CHANGED INFORMATION
The information provided on the Form |
|
|
is amended as follows: |
|
|
|
|
|
|
|
Change From |
|
Change To |
|
|
Employee Name |
|
|
|
SSN or Board Tracking #
Date of Injury
County of Injury
Reasons for change(s) above:
B. CERTIFICATION
I certify that I have today sent a copy of this form to all parties in this claim and to the State Board of Workers’ Compensation, 270 Peachtree Street, NW, Atlanta, Georgia
Print name here
Address
Signature
City
State
Zip Code
GA Bar number
Phone Number
Date
IF YOU HAVE QUESTIONS PLEASE CONTACT THE STATE BOARD OF WORKERS’ COMPENSATION AT
WILLFULLY MAKING A FALSE STATEMENT FOR THE PURPOSE OF OBTAINING OR DENYING BENEFITS IS A CRIME SUBJECT TO PENALTIES OF UP TO $10,000.00 PER VIOLATION (O.C.G.A.
REVISION . 07/2011 |
14a |
REQUEST TO CHANGE INFORMATION |
|
ON A PREVIOUSLY FILED FORM |