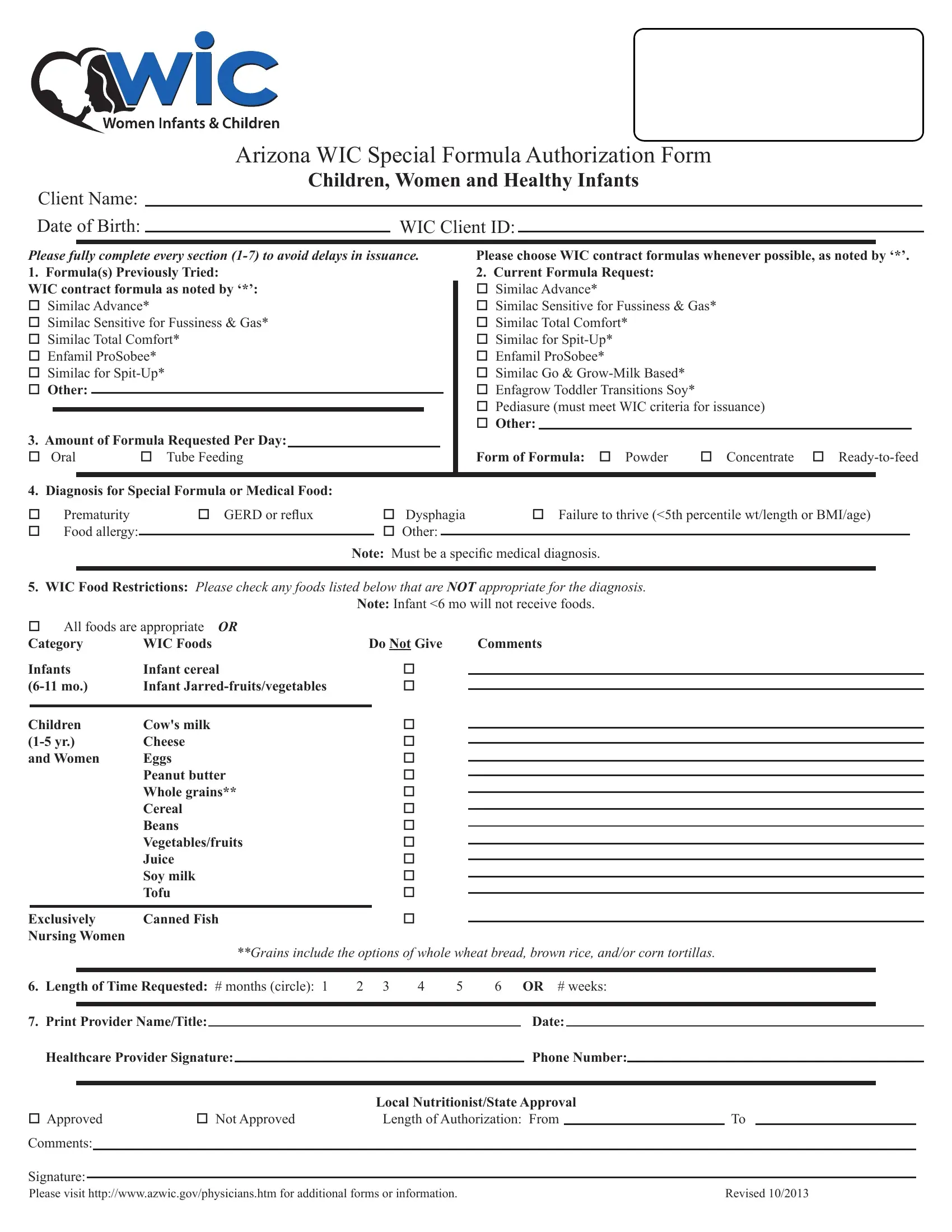
The Arizona WIC Special Formula Authorization Form is a critical document designed to facilitate access to special formula and medical foods for children, women, and healthy infants who are part of the Women, Infants, and Children (WIC) program. The form requires detailed information to be filled out in sections 1-7, ensuring a comprehensive assessment of the client's needs to prevent any delays in the issuance of the required nutritional products. It lists specific formulas, including WIC contract formulas marked with an asterisk, for different conditions such as fussiness, gas, or digestive issues, and asks for the quantity of formula needed per day. Furthermore, it asks for a diagnosis that justifies the need for a special formula or medical food, highlighting the importance of a specific medical diagnosis. Dietary restrictions related to the diagnosis are also addressed, indicating which WIC-provided foods are not suitable for the client. The form specifies the duration for which the special formula is requested, and it must be completed and signed by a healthcare provider, indicating the necessity of professional input. It also outlines a process for approval by a local nutritionist or state authority, ensuring that the request is evaluated thoroughly. This form thus plays a pivotal role in making sure that individuals under the WIC program receive the specialized nutritional support they need, based on their unique health requirements.
| Question | Answer |
|---|---|
| Form Name | Wic Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wic form pdf, printable wic forms, wic arizona form, wic program arizona form |
|
|
Arizona WIC Special Formula Authorization Form |
|
|||
|
|
Children, Women and Healthy Infants |
|
|||
Client Name: |
|
|
|
|
|
|
Date of Birth: |
|
WIC Client ID: |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Please fully complete every section
1.Formula(s) Previously Tried:
WIC contract formula as noted by ‘*’: o Similac Advance*
o Similac Sensitive for Fussiness & Gas* o Similac Total Comfort*
o Enfamil ProSobee* o Similac for
3. Amount of Formula Requested Per Day:
o Oral |
o Tube Feeding |
Please choose WIC contract formulas whenever possible, as noted by ‘*’.
2.Current Formula Request: o Similac Advance*
o Similac Sensitive for Fussiness & Gas* o Similac Total Comfort*
o Similac for
o Similac Go &
o Pediasure (must meet WIC criteria for issuance) o Other:
Form of Formula: o Powder |
o Concentrate o |
4. Diagnosis for Special Formula or Medical Food: |
|
|
|
||
o |
Prematurity |
o GERD or relux |
o Dysphagia |
o Failure to thrive (<5th percentile wt/length or BMI/age) |
|
o |
Food allergy: |
|
o Other: |
|
|
|
|
|
|||
Note: Must be a speciic medical diagnosis.
5.WIC Food Restrictions: Please check any foods listed below that are NOT appropriate for the diagnosis.
Note: Infant <6 mo will not receive foods.
o All foods are appropriate OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Category |
WIC Foods |
Do Not Give |
|
Comments |
|
|
|
|
||||||||||||
Infants |
Infant cereal |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
|||||
Infant |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
|
Children |
Cow's milk |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Cheese |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
and Women |
Eggs |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
Peanut butter |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Whole grains** |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Cereal |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Beans |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Vegetables/fruits |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Juice |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Soy milk |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Tofu |
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
o |
|
|
|
|
|
|
|
|
|
|
|
||
Exclusively |
Canned Fish |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Nursing Women |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
**Grains include the options of whole wheat bread, brown rice, and/or corn tortillas. |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. Length of Time Requested: # months (circle): 1 |
2 3 |
4 |
5 |
6 OR # weeks: |
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
7. Print Provider Name/Title: |
|
|
|
|
|
|
|
|
Date: |
|
|
|
|
|
|
|||||
|
Healthcare Provider Signature: |
|
|
|
|
|
|
|
Phone Number: |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Local Nutritionist/State Approval |
|
|
|
|
||||||||
o Approved |
o Not Approved |
|
Length of Authorization: From |
|
|
|
To |
|
|
|
||||||||||
Comments:
Signature:
Please visit http://www.azwic.gov/physicians.htm for additional forms or information. |
Revised 10/2013 |