
When you would like to fill out wic referral form, you won't have to download and install any sort of programs - simply make use of our PDF tool. To maintain our tool on the cutting edge of practicality, we aim to put into operation user-driven features and improvements on a regular basis. We're routinely looking for feedback - assist us with remolding PDF editing. Here is what you'll want to do to start:
Step 1: Access the PDF file inside our tool by pressing the "Get Form Button" in the top area of this webpage.
Step 2: With this handy PDF editing tool, you can actually do more than just complete blanks. Express yourself and make your docs appear sublime with customized textual content added, or adjust the original content to excellence - all that backed up by the capability to incorporate stunning pictures and sign the file off.
This PDF doc will need specific information; in order to ensure consistency, you should take note of the next guidelines:
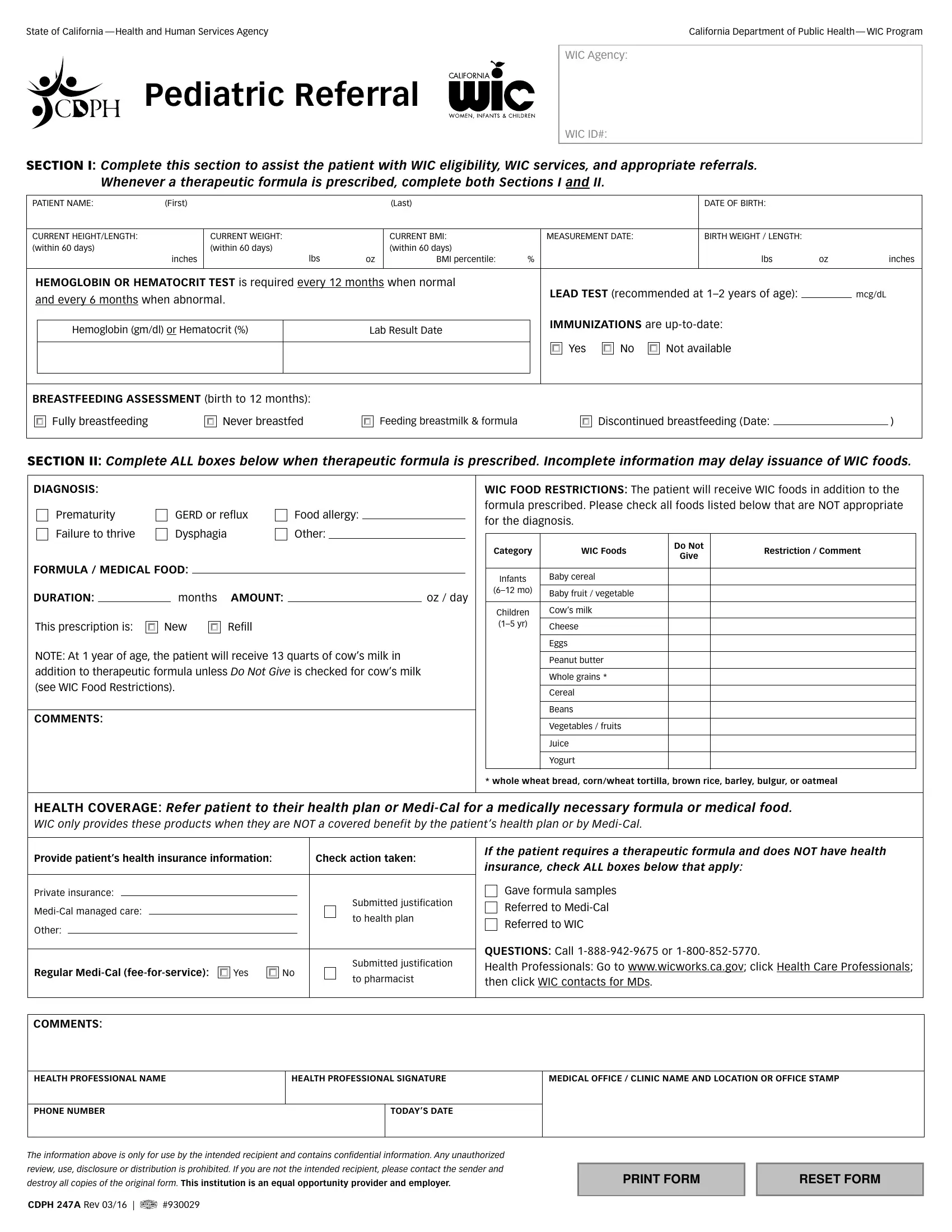
1. The wic referral form requires certain details to be inserted. Make sure the following blanks are complete:
2. Once your current task is complete, take the next step – fill out all of these fields - Prematurity, GERD or reflux, Food allergy, Failure to thrive, Dysphagia, Other, FORMULA MEDICAL FOOD, DURATION, months AMOUNT, oz day, This prescription is, New, Refill, NOTE At year of age the patient, and COMMENTS with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing COMMENTS, HEALTH PROFESSIONAL NAME, HEALTH PROFESSIONAL SIGNATURE, MEDICAL OFFICE CLINIC NAME AND, PHONE NUMBER, TODAYS DATE, The information above is only for, review use disclosure or, destroy all copies of the original, CDPH A Rev, PRINT FORM, and RESET FORM is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Be very mindful when completing COMMENTS and MEDICAL OFFICE CLINIC NAME AND, because this is where many people make some mistakes.
Step 3: Before submitting the document, check that all blank fields are filled in the right way. The moment you’re satisfied with it, click on “Done." Grab your wic referral form the instant you register online for a 7-day free trial. Readily access the pdf file inside your personal account, with any edits and changes automatically preserved! FormsPal guarantees protected form completion without personal information record-keeping or sharing. Be assured that your data is in good hands here!