WISCONSIN DEPARTMENT OF HEALTH SERVICES
Division of Health Care Access and Accountability F-10138 (07/08)
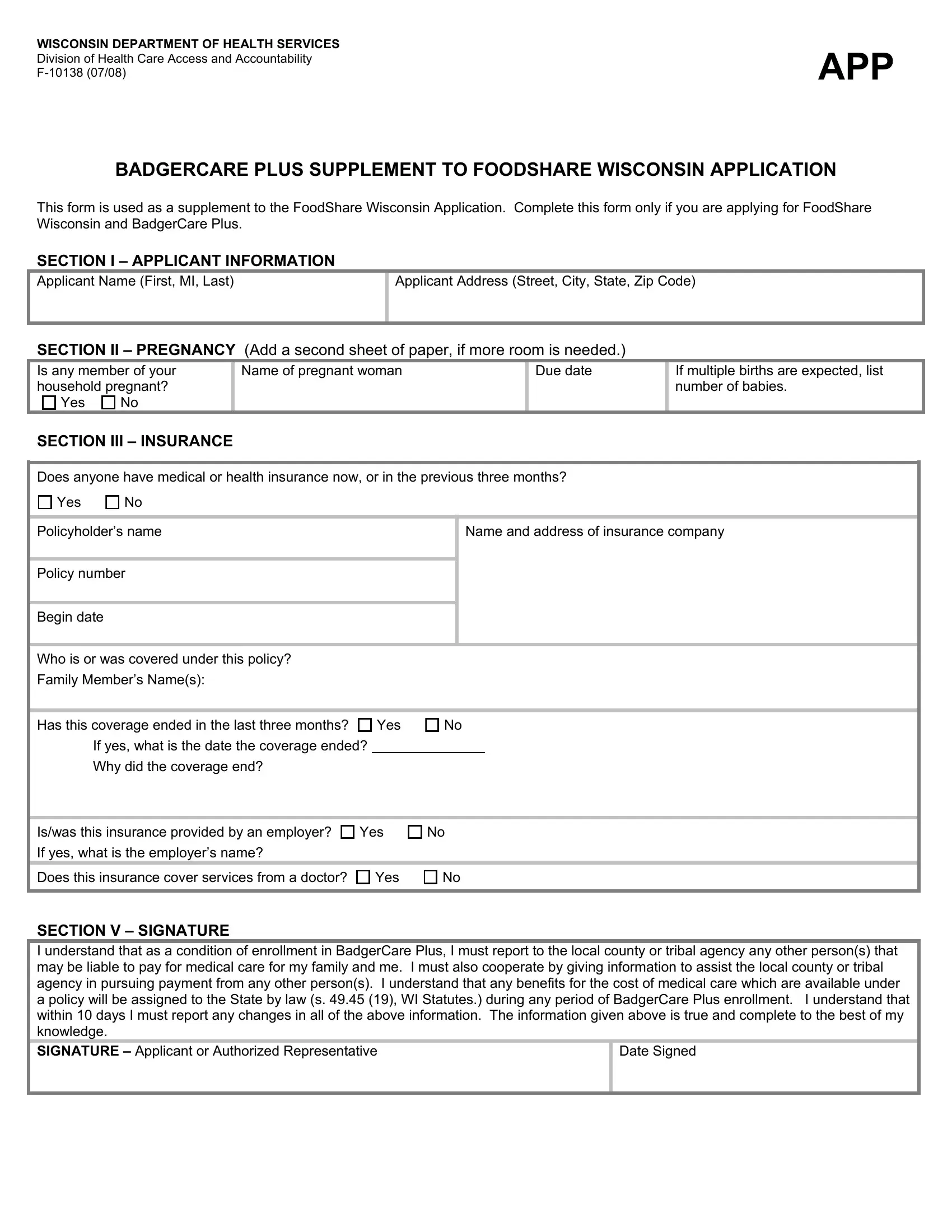
BADGERCARE PLUS SUPPLEMENT TO FOODSHARE WISCONSIN APPLICATION
This form is used as a supplement to the FoodShare Wisconsin Application. Complete this form only if you are applying for FoodShare Wisconsin and BadgerCare Plus.
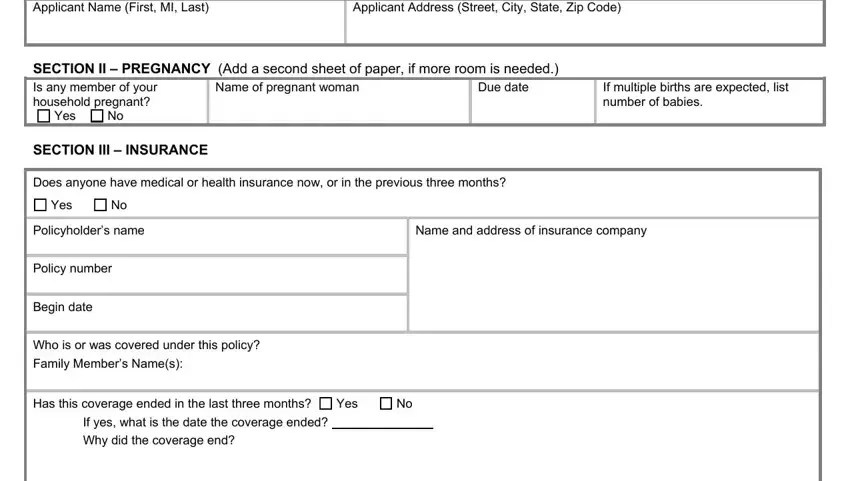
SECTION I – APPLICANT INFORMATION
Applicant Name (First, MI, Last)
Applicant Address (Street, City, State, Zip Code)
SECTION II – PREGNANCY (Add a second sheet of paper, if more room is needed.)
Is any member of your household pregnant? Yes No
If multiple births are expected, list number of babies.
SECTION III – INSURANCE
Does anyone have medical or health insurance now, or in the previous three months?
Policyholder’s name
Policy number
Begin date
Name and address of insurance company
Who is or was covered under this policy?
Family Member’s Name(s):
Has this coverage ended in the last three months?
If yes, what is the date the coverage ended?
Why did the coverage end?
Is/was this insurance provided by an employer?
If yes, what is the employer’s name?
Does this insurance cover services from a doctor?
SECTION V – SIGNATURE
I understand that as a condition of enrollment in BadgerCare Plus, I must report to the local county or tribal agency any other person(s) that may be liable to pay for medical care for my family and me. I must also cooperate by giving information to assist the local county or tribal agency in pursuing payment from any other person(s). I understand that any benefits for the cost of medical care which are available under a policy will be assigned to the State by law (s. 49.45 (19), WI Statutes.) during any period of BadgerCare Plus enrollment. I understand that within 10 days I must report any changes in all of the above information. The information given above is true and complete to the best of my knowledge.
SIGNATURE – Applicant or Authorized Representative
BADGERCARE PLUS SUPPLEMENT TO FOODSHARE WISCONSIN APPLICATION
F-10138 (07/08)
RIGHTS AND RESPONSIBILITIES
Your signature on the application means that you understand and acknowledge that the local county or tribal agency and the state Department of Health Services is authorized to request any information that is appropriate and necessary for the proper administration of BadgerCare Plus as authorized under Wisconsin law.
Any person, including any financial institution, credit reporting agency, employer, or educational institution, is authorized to release this information, according to Wisconsin Statute s. 49.22(2m)(a): “The Department may request from any person in this state information it determines appropriate and necessary for the administration of this section, ss.49.141 to 49.161, 49.19, 49.46, 49.468 and 49.47 and programs carrying out the purposes of 7 USC 2011 to 2029. Unless access to the information is prohibited or restricted by law, or unless the person has good cause, as determined by the Department in accordance with federal law and regulations, for refusing to cooperate, the person shall make a good faith effort to provide this information within 7 days after receiving a request under this paragraph. Except as provided in subs. (2p) and (2r) and subject to sub.(12), the Department or the county child support agency under s.59.53(5) may disclose information obtained under this paragraph only in the administration of this section, ss.49.141 to 49.161, 49.19, 49.46 and 49.47 and programs carrying out the purposes of 7 USC 2011 to 2029. Employees of the department or a county child support agency under s.59.53(5) are subject to s.49.83.”
You have the right to appeal any action taken concerning your BadgerCare Plus, or Family Planning services application or on going benefits that you do not agree with by requesting a Fair Hearing. You may request a Fair Hearing by calling or writing to:
Wisconsin Department of Administration
Division of Hearings and Appeals
P.O. Box 7875
Madison, WI 53707-7875
Telephone: (608) 266-3096
You can download the “Request For a Fair Hearing” form from the Division of Hearing and Appeals Web site at http://dha.state.wi.us/home/.
You may also contact your local agency and ask for a Fair Hearing verbally or in writing.
The Department of Health Services (DHFS) is an equal opportunity employer and service provider. For civil rights questions, CALL (608) 266-9372 (voice) or (888) 701-1251 (TTY).
To file a complaint of discrimination by contacting either the:
•Wisconsin Department of Health Services (DHFS)
Affirmative Action and Civil Rights Compliance Office
1 W. Wilson, Room 555
Madison, WI 53707-7850
Telephone: (608) 266-9372 (Voice); (888) 701-1251 (TTY)
Fax: (608) 267-2147
•U.S. Department of Health and Human Services Office for Civil Rights – Region V 233 N. Michigan Avenue
Suite 240 Chicago, IL 60601
Telephone: (312) 886-5077 (voice) or (312) 353-5693 (TTY)