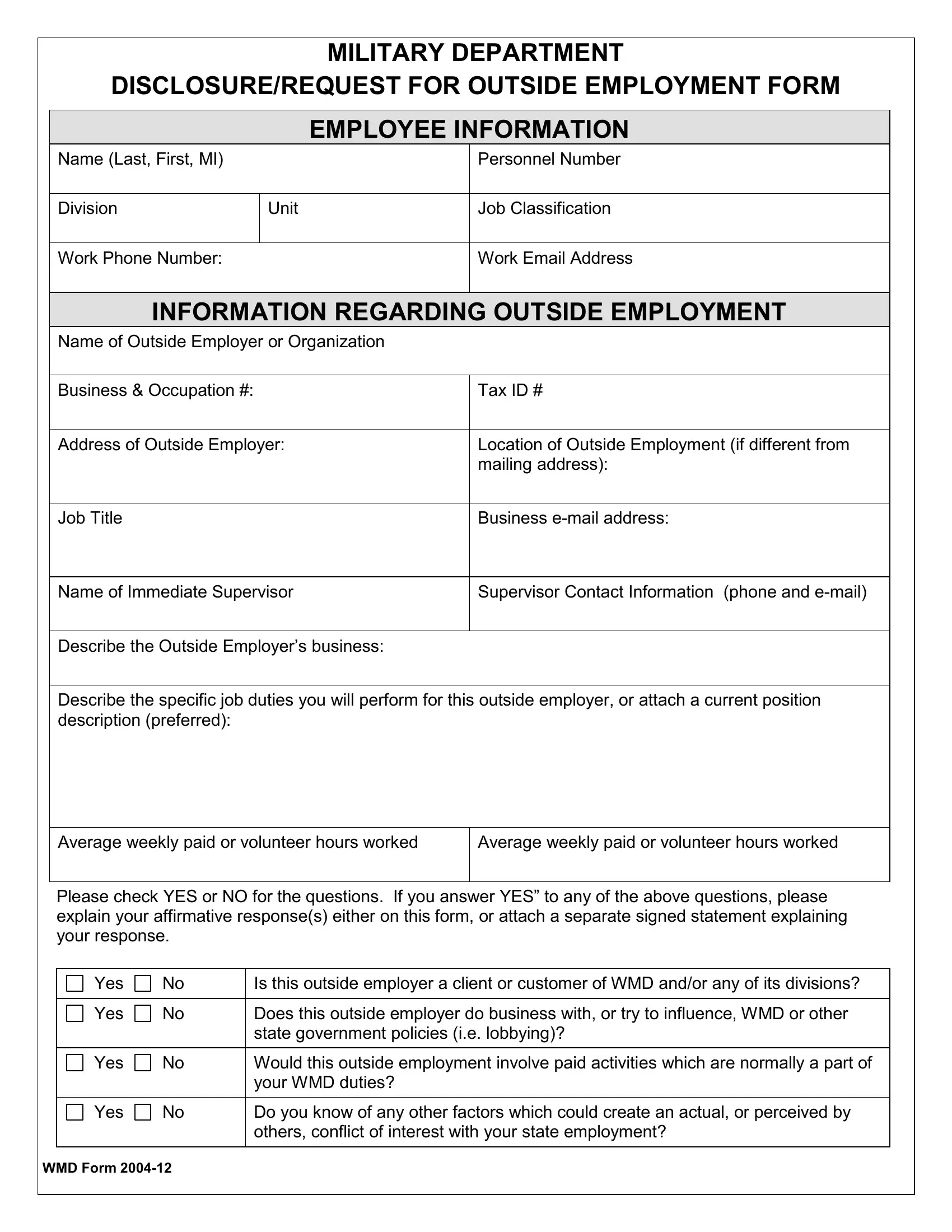
In an era where operational transparency and conflict of interest mitigation are paramount, the WMD Form 2004-12 serves as a crucial document for members of the Military Department seeking to engage in outside employment. This comprehensive form mandates the disclosure of detailed employee information, including but not limited to name, personnel number, division, unit, job classification, and contact details. Furthermore, it requires the submission of extensive details pertaining to the proposed outside employment, including the employer's name, business and occupation number, Tax ID, job title, supervisor information, and a thorough description of job duties. Perhaps most critically, the form contains a set of pivotal questions aimed at identifying potential conflicts of interest, probing into whether the outside employment intersects with the employee's duties at the Military Department, or involves a business or entity that could influence or conduct operations regulated by the department. Approval process details are meticulously outlined, including steps for supervisor, manager, EMT Director, HR Director, and possibly Director (TAG) review, highlighting the layered oversight mechanism adopted by the department. Employees are reminded of the necessity of honesty and completeness in their disclosure, underlining the form's role in maintaining the integrity of both the individual's and the department's professional responsibilities. By incorporating such exhaustive details and procedural steps, the WMD Form 2004-12 embodies the department's commitment to ethical conduct and the avoidance of conflicts of interest in its workforce's engagements beyond their primary employment.
| Question | Answer |
|---|---|
| Form Name | Wmd Form 2004 12 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sample of usa military form, military registration form, soldiers forms, what to do when applying military forms |
MILITARY DEPARTMENT
DISCLOSURE/REQUEST FOR OUTSIDE EMPLOYMENT FORM
|
|
EMPLOYEE INFORMATION |
|
Name (Last, First, MI) |
|
|
Personnel Number |
|
|
|
|
Division |
Unit |
|
Job Classification |
|
|
|
|
Work Phone Number: |
|
|
Work Email Address |
|
|
|
|
INFORMATION REGARDING OUTSIDE EMPLOYMENT
Name of Outside Employer or Organization
Business & Occupation #: |
Tax ID # |
|
|
Address of Outside Employer: |
Location of Outside Employment (if different from |
|
mailing address): |
|
|
Job Title |
Business |
|
|
Name of Immediate Supervisor |
Supervisor Contact Information (phone and |
|
|
Describe the Outside Employer’s business:
Describe the specific job duties you will perform for this outside employer, or attach a current position description (preferred):
Average weekly paid or volunteer hours worked |
Average weekly paid or volunteer hours worked |
|
|
Please check YES or NO for the questions. If you answer YES” to any of the above questions, please explain your affirmative response(s) either on this form, or attach a separate signed statement explaining your response.
Yes |
No |
Is this outside employer a client or customer of WMD and/or any of its divisions? |
|
|
|
Yes |
No |
Does this outside employer do business with, or try to influence, WMD or other |
|
|
state government policies (i.e. lobbying)? |
|
|
|
Yes |
No |
Would this outside employment involve paid activities which are normally a part of |
|
|
your WMD duties? |
|
|
|
Yes |
No |
Do you know of any other factors which could create an actual, or perceived by |
|
|
others, conflict of interest with your state employment? |
|
|
|
WMD FORM
Yes |
No |
Does this outside employer conduct operations, or activities, which are regulated |
|
|
by WMD? |
|
|
|
Explanation for areas in which you marked yes on the previous page (attach additional pieces of paper if necessary).
By my signature, I certify that this information is true and complete to the best of my knowledge. I also certify that I I have read and understand Washington Military Department Policy
|
|
|
|
|
|
|
|
|
|
|
|
NAME: |
|
|
|
DATE: |
|
|
|
|
|
|
|
|
|
APPROVAL PROCESS |
|
|
|
|||
|
Office / Function |
|
|
Recommendation |
|
Signature |
|
Date |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Approval |
|
|
|
|
|
|
|
Supervisor |
|
|
Approved with noted conditions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Disapproval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Approval |
|
|
|
|
|
|
|
|
|
|
Approved with noted conditions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Manager |
|
|
|
|
|
|
|
|
|
|
|
|
Disapproval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
APPROVAL |
|
|
|
|
||
|
|
|
|
Approval |
|
|
|
|
|
|
|
EMT Director |
|
|
Approved with noted conditions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Disapproval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Approval |
|
|
|
|
|
|
|
HR Director |
|
|
Approved with noted conditions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
Disapproval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
Director (TAG) Review |
|
|
Approval |
|
|
|
|
|
|
|
(if required) |
|
|
Approved with noted conditions |
|
|
|
|
|
|
|
|
|
|
Disapproval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comments: |
|
|
|
|
|
|
|
|
|
|
cc:Payroll file Personnel file
WMD FORM