It won't be challenging to get wyequalitycare through our PDF editor. Here's how you will be able rapidly develop your template.
Step 1: The web page has an orange button that says "Get Form Now". Please click it.
Step 2: You will discover all of the options you can take on your document when you have entered the wyequalitycare editing page.
Complete the following segments to prepare the file:
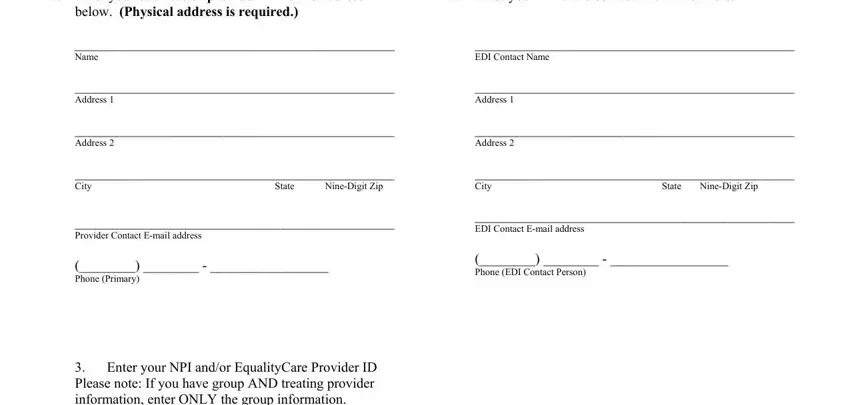
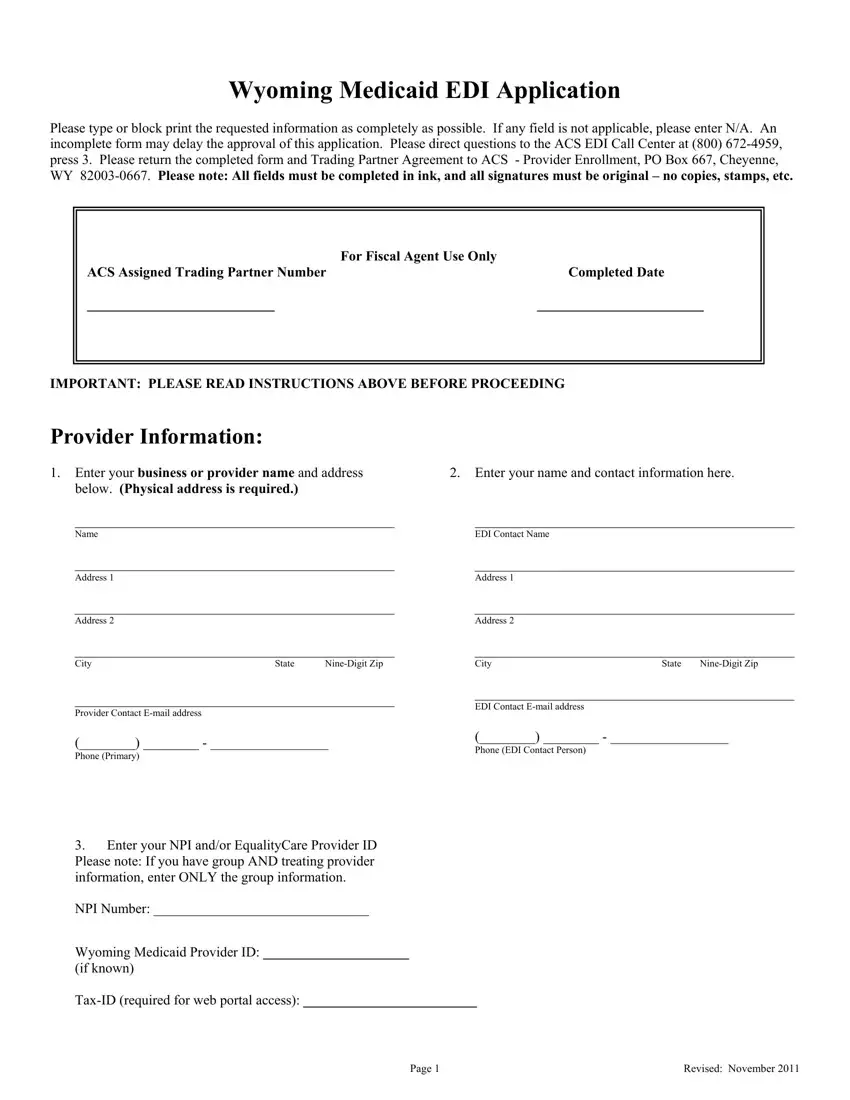
Type in the information in the Enter your NPI andor EqualityCare, NPI Number, Wyoming Medicaid Provider ID, if known, TaxID required for web portal, Page, and Revised November area.
Jot down the expected data when you find yourself within the I will retrieve my deliver to, A third party eg clearinghouse, I do not wish to use the at this, My files are ALREADY being, to this trading partner number and, trading partner name and number, and effective date change is effective part.
Describe the rights and obligations of the sides inside the field If you or your organization is, If you are not already submitting, Billing Agent, Billing Agent Trading Partner ID, Clearinghouse, Clearinghouse Trading Partner ID, Vendor Supplied Software, Vendor Software Trading Partner ID, Secure Web Portal free webbased, httpwyequalitycareacsinccom, WINASAP Billing Software free, Download the software from, mailed to you instead, and Agreement.
End by reviewing all of these areas and submitting the pertinent information: G Trading Partner may provide, for any purpose other, solely, H Agreement contains, the entire agreement between the, I Submitter may elect to execute, SUBMITTER, Provider NumberTrading Partner ID, Signature, Printed Name and Title, Date, and Mail Completed Agreement To.
Step 3: Press "Done". You can now transfer the PDF document.
Step 4: You will need to create as many copies of your form as you can to remain away from possible issues.
