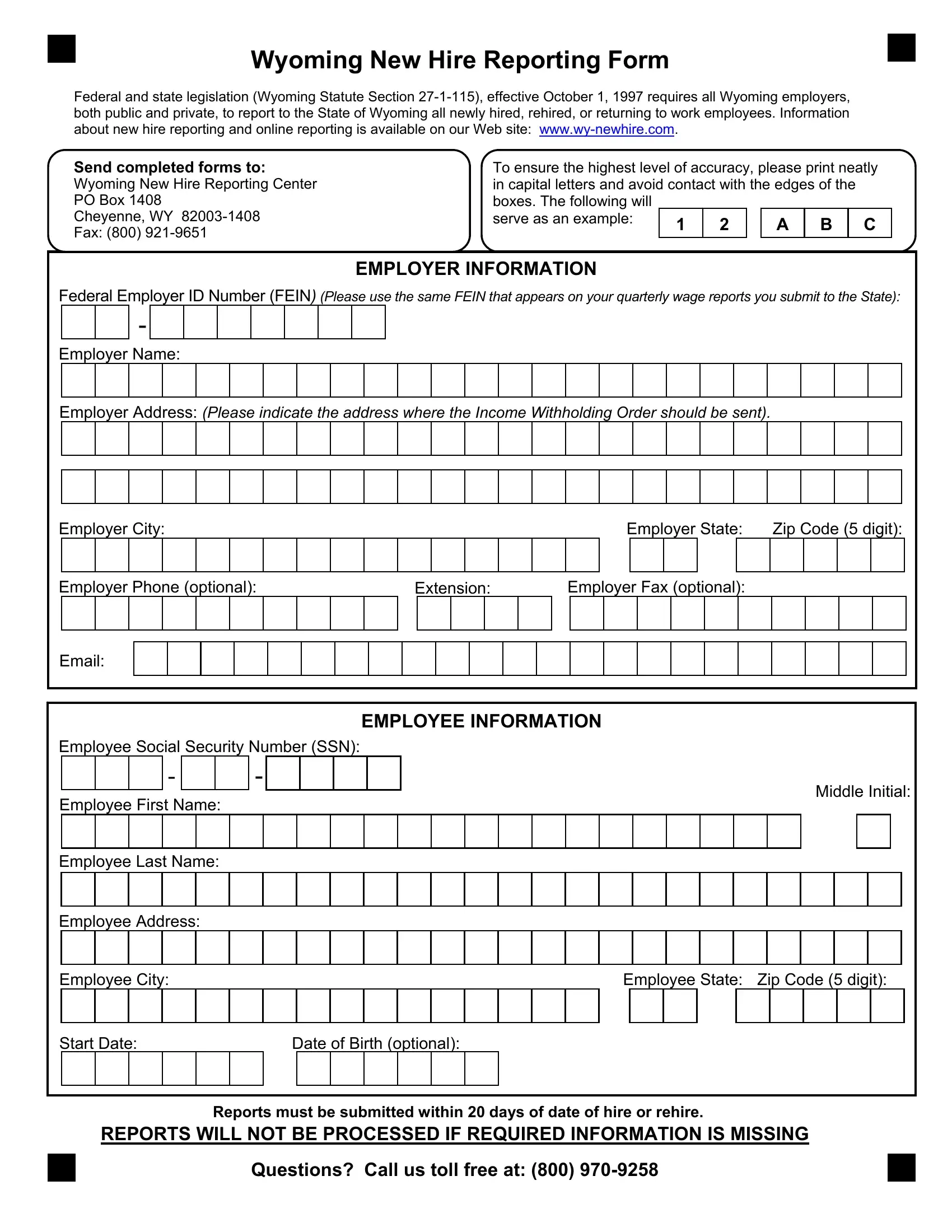
Since October 1, 1997, in alignment with federal and state legislation (Wyoming Statute Section 27-1-115), every employer in Wyoming, regardless of being in the public or private sector, is mandated to submit details regarding all newly hired, rehired, or employees returning to work through the Wyoming New Hire Reporting Form. This obligation underscores the importance of maintaining a transparent and updated employment record system, facilitating efficient income withholding order processing among other legal and administrative processes. Employers are guided to ensure the accuracy and completeness of each submission by printing clearly in capital letters to prevent errors. The form requires comprehensive employer and employee information, including but not limited to the Federal Employer ID Number (FEIN), the employer's name and address, as well as the employee's social security number, name, address, and job start date. Moreover, a deadline is set for these reports to be submitted within 20 days from the employee's hiring date, emphasizing the promptness in compliance. For additional assistance, employers have access to online resources at www.wy-newhire.com and can reach out through a toll-free number. This structured approach not only simplifies the reporting process but also ensures the state's labor force data remains current, supporting several statutory and administrative functions.
| Question | Answer |
|---|---|
| Form Name | Wyoming New Hire Reporting Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | wyoming hire latest, wyoming workers compensation new hire reporting, wyoming new reporting, wy new hire reporting |
Wyoming New Hire Reporting Form
Federal and state legislation (Wyoming Statute Section
Send completed forms to: Wyoming New Hire Reporting Center PO Box 1408
Cheyenne, WY
To ensure the highest level of accuracy, please print neatly
in capital letters and avoid contact with the edges of the |
|
||||
boxes. The following will |
|
|
|
|
|
serve as an example: |
1 |
2 |
A |
B |
C |
|
|||||
EMPLOYER INFORMATION
Federal Employer ID Number (FEIN) (Please use the same FEIN that appears on your quarterly wage reports you submit to the State):
-
Employer Name:
Employer Address: (Please indicate the address where the Income Withholding Order should be sent).
Employer City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employer State: |
|
Zip Code (5 digit): |
|||||||||||||||||||
Employer Phone (optional): |
|
|
|
|
|
|
|
|
|
Extension: |
|
Employer Fax (optional): |
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
Email: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYEE INFORMATION |
|
|
|
|
|
|
||||||||||||||||||||||||||||
Employee Social Security Number (SSN): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
- |
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Middle Initial: |
||||||||||
|
Employee First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Employee Last Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Employee Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Employee State: |
Zip Code (5 digit): |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
START Date: |
|
|
|
Date of Birth (optional): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Reports must be submitted within 20 days of date of hire or rehire.
REPORTS WILL NOT BE PROCESSED IF REQUIRED INFORMATION IS MISSING
Questions? Call us toll free at: (800)