
You'll be able to prepare clinical intake interview form effectively with our PDFinity® PDF editor. Our editor is continually developing to give the very best user experience possible, and that's thanks to our dedication to constant enhancement and listening closely to customer feedback. Starting is easy! All you need to do is adhere to the following basic steps down below:
Step 1: Hit the orange "Get Form" button above. It's going to open up our tool so that you can start filling in your form.
Step 2: This editor grants the opportunity to modify PDF forms in various ways. Change it with any text, correct what's already in the document, and add a signature - all readily available!
As a way to finalize this PDF document, make sure you type in the necessary details in each area:
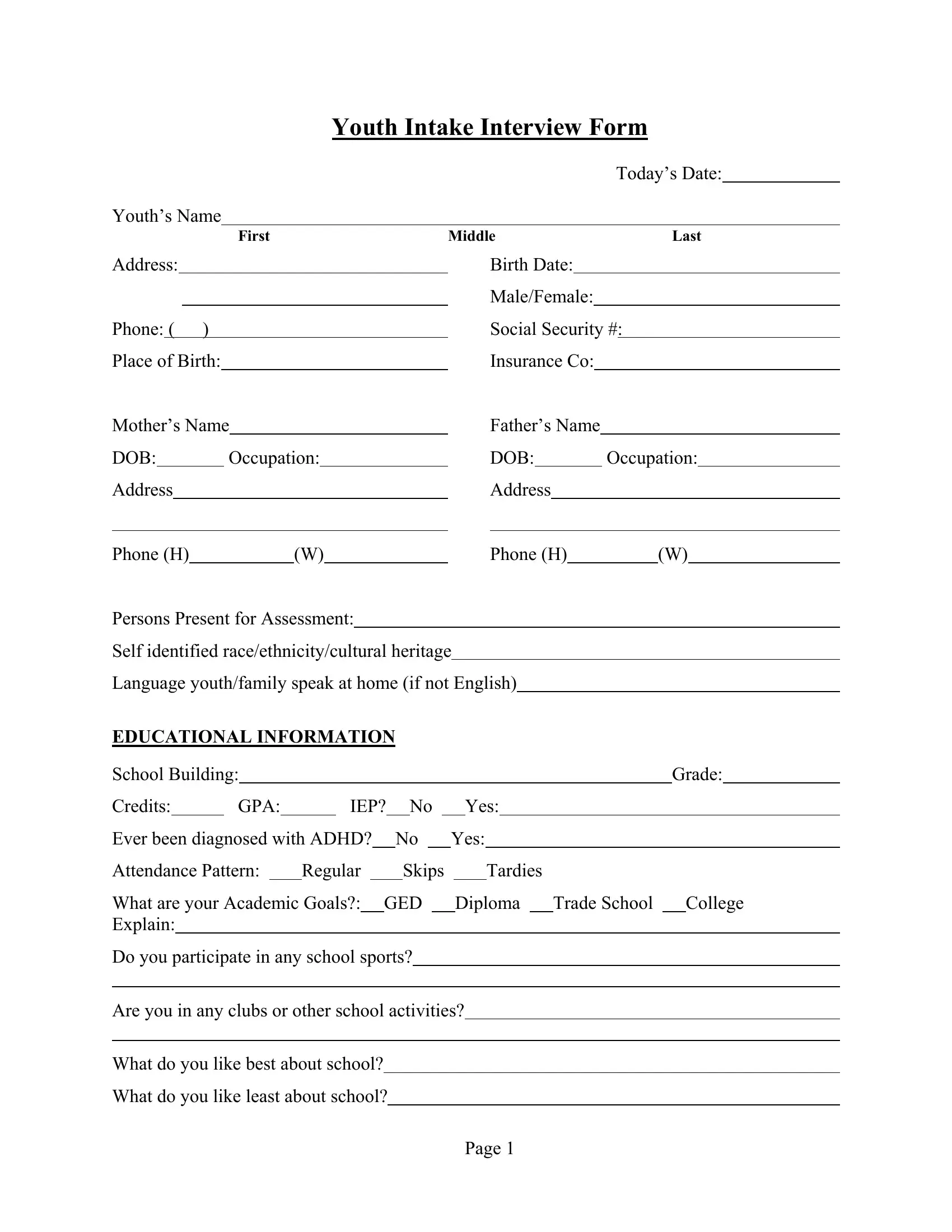
1. Fill out the clinical intake interview form with a selection of essential blanks. Gather all the important information and make certain absolutely nothing is overlooked!
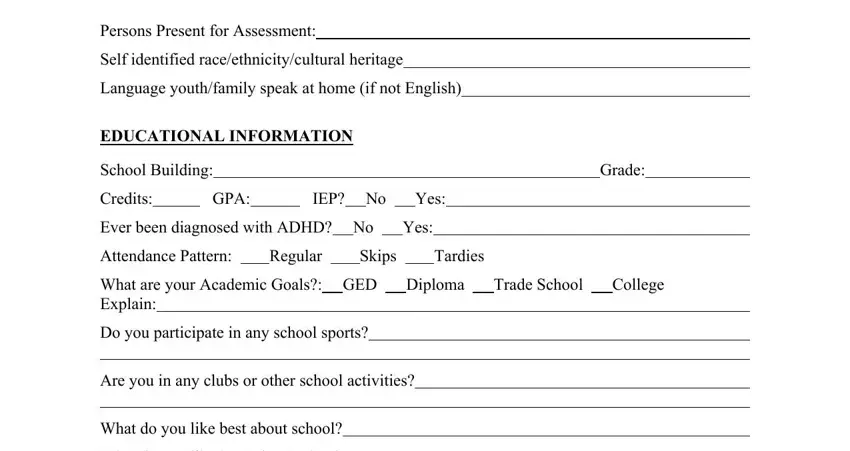
2. Just after this section is filled out, go to type in the relevant details in all these: Persons Present for Assessment, Self identified, Language youthfamily speak at home, EDUCATIONAL INFORMATION School, Credits, GPA, IEP No Yes, Ever been diagnosed with ADHD No, Attendance Pattern Regular Skips, Grade, What are your Academic Goals GED, Do you participate in any school, Are you in any clubs or other, and What do you like best about school.
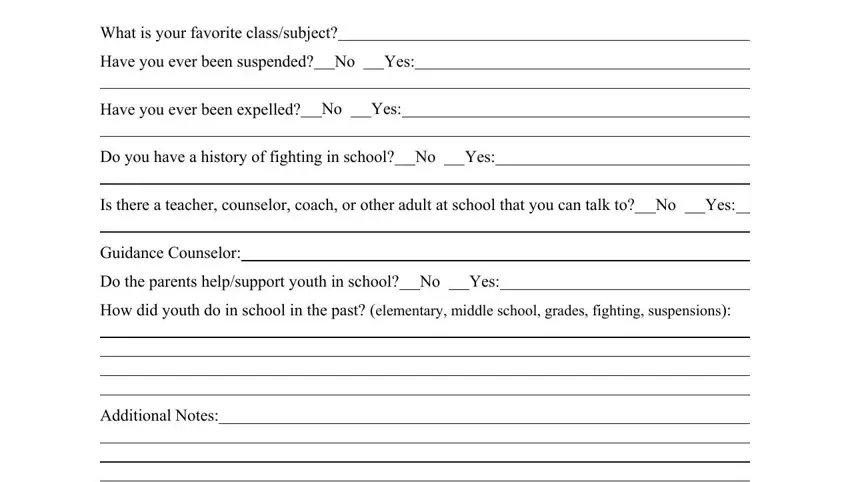
3. Completing What is your favorite classsubject, Have you ever been suspended No Yes, Have you ever been expelled No Yes, Do you have a history of fighting, Is there a teacher counselor coach, Guidance Counselor, Do the parents helpsupport youth, How did youth do in school in the, and Additional Notes FAMILY is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
People frequently get some points wrong when completing Additional Notes FAMILY in this part. Ensure you read twice whatever you enter here.
4. Filling out Additional Notes FAMILY, Relatives Other, Legal Adoption, Stepfather Stepmother, Who else lives in the home, Home Environment, Describe the relationships and, and What are your rules at home is paramount in the fourth form section - you should definitely devote some time and fill out each blank!
5. The pdf must be completed with this particular area. Further you'll see a detailed list of blank fields that need accurate information for your form usage to be complete: What consequences do you typically, What consequences did you face at, What are some things you do, Significant family events traumas, What are some strengths you have, What adult do you spend most of, Relationship, Name, Which extended family members, Relationship, Name, History of running away No Yes How, and Any previous out of home placements.
Step 3: Right after you've looked once more at the details in the file's blank fields, just click "Done" to conclude your form. Make a 7-day free trial subscription with us and gain direct access to clinical intake interview form - download or edit from your personal account. FormsPal is dedicated to the privacy of our users; we make sure all personal data going through our system continues to be protected.