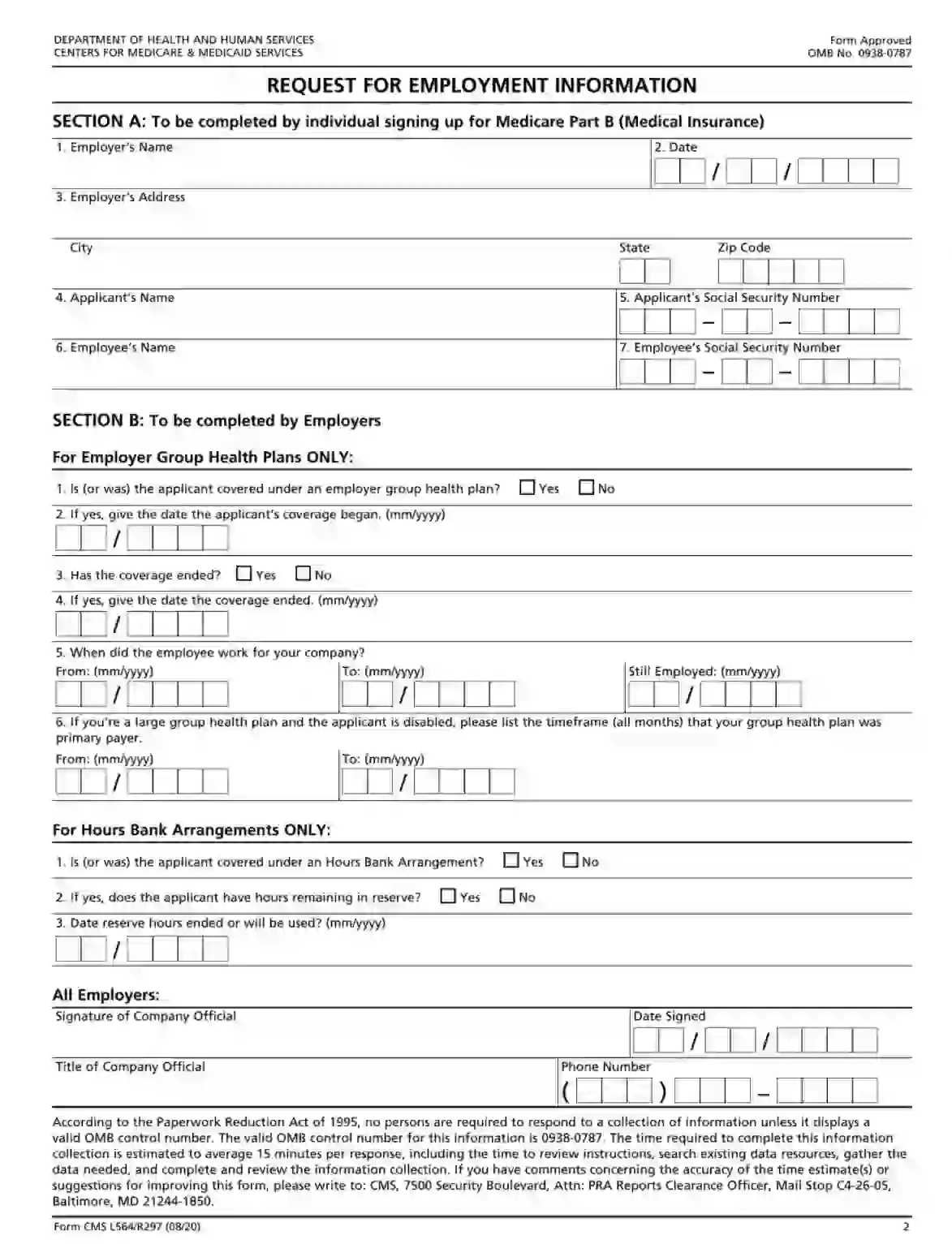
CMS L564-R297, also known as “Request for Employment Information,” is designed for individuals who are applying for Medicare and are seeking to qualify for the premium-free Part A based on their employment history or that of a spouse. The CMS L564-R297 is filled out by the applicant’s employer or the employer of the spouse, and it verifies the employment and health insurance coverage details necessary to establish eligibility for premium-free Medicare Part A, which is generally available without a premium to those who have paid Medicare taxes for a sufficient number of quarters during their working years.
This template is quite easy, and highly likely, you will not need any additional help to create it. Workers have to complete the template’s first part (Section A) and then pass their document to the employers to fill out their block (Section B).
The template is available online; you are not required to order it from anywhere. Although CMS offers the current version on their official site, we suggest using our advanced form-building software for generating legal templates, including the Form CMS-L564, just in a moment.
When the template is downloaded, you can open it and start inserting information there. Use our manual to see how to create the document properly and what to include there.
Enter the Worker’s Data
As you already know, the first section must be completed by applicants or workers. A worker must enter their employer’s name in the first line, then write the date when the form is created on the right. The next field is for the employer’s full address, including the state and postal code.
Below, you shall write your full name and social security number (as an applicant). Under this line, you must indicate the “employee’s” name: either your name or the name of the one whose insurance is covered by the employer (if you are a spouse or a relative of this person and are applying for insurance).

Pass the Papers to the Employer
Now your work is done, and you need to transfer the document to the employer to finish the filling-out process.
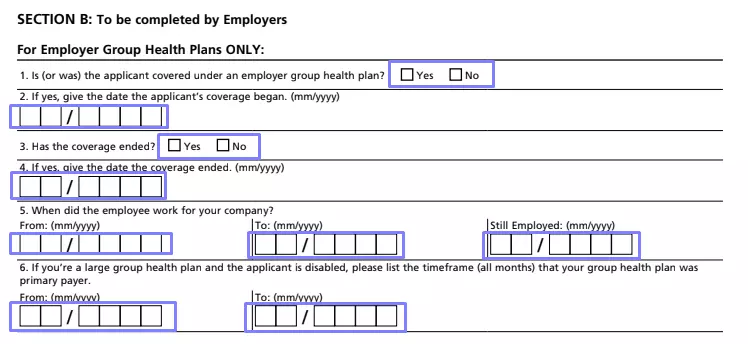
As an employer, you must choose between employer group health plans or hours bank arrangements (it depends on the insurance program you have chosen before).
If you need to fill out the first part, state if the applicant is or was covered under the Group Health Plan or not. Mark the suitable box by a cross or tick. If the answer is positive, enter the date when the coverage started. Then, specify if it has already finished (if yes, add the date, too).
Give the terms when the employee was working for your entity (the first and the last day). For workers who are still in your company, write the current date in the relevant line on the right.
Some entities use large group plans due to the entity’s size. If this is the used plan, your applicant is disabled, and the plan was the key payer for your applicant’s medical service for a specific period, write the period here.
If the second part is chosen, indicate whether the applicant is or was covered with the use of the Hours Bank Arrangement. Answer if there are still reserved hours for the applicant (a “yes” or “no” question). Below, you have to insert the date until these hours remain valid (if there are any). You should write only the month and year.

Sign the Document
It does not matter which insurance your company uses; you as an employer must sign the form. Write your title under your signature, enter the date of signing, and type your phone number on the block’s right-hand side.