DD Form 2870, also known as the “Authorization for Disclosure of Medical or Dental Information,” allows military personnel to authorize the release of their medical and dental records to designated parties. The primary purpose of DD Form 2870 is to facilitate the sharing of sensitive health information in compliance with privacy regulations. It is essential for situations where military personnel need to provide proof of medical conditions for claims, continue medical care with civilian providers, or support other personal or family matters.
Other DOD Forms
Need other DOD PDF forms? Check the list following next to see what you are able to fill out and edit with FormsPal. Also, keep in mind that you can upload, fill out, and edit any PDF document at FormsPal.
After the patient or their legal representative (including the parent) completes the paper, the patient needs to serve DD Form-2870 to FAHC’s Records Window personally. This requirement is compulsory to protect the patient’s confidential information.
Still, there are cases when the declarant cannot render the completed form in person. In these circumstances, they may follow one of two possible algorithms:
Also, the patient must include a copy of one of the afore-mentioned ID cards.
These strict measures will support the security aspect and help validate the patient’s signature. If you don’t have any of the mentioned ID cards, you can submit a copy of any state or government photo ID document.
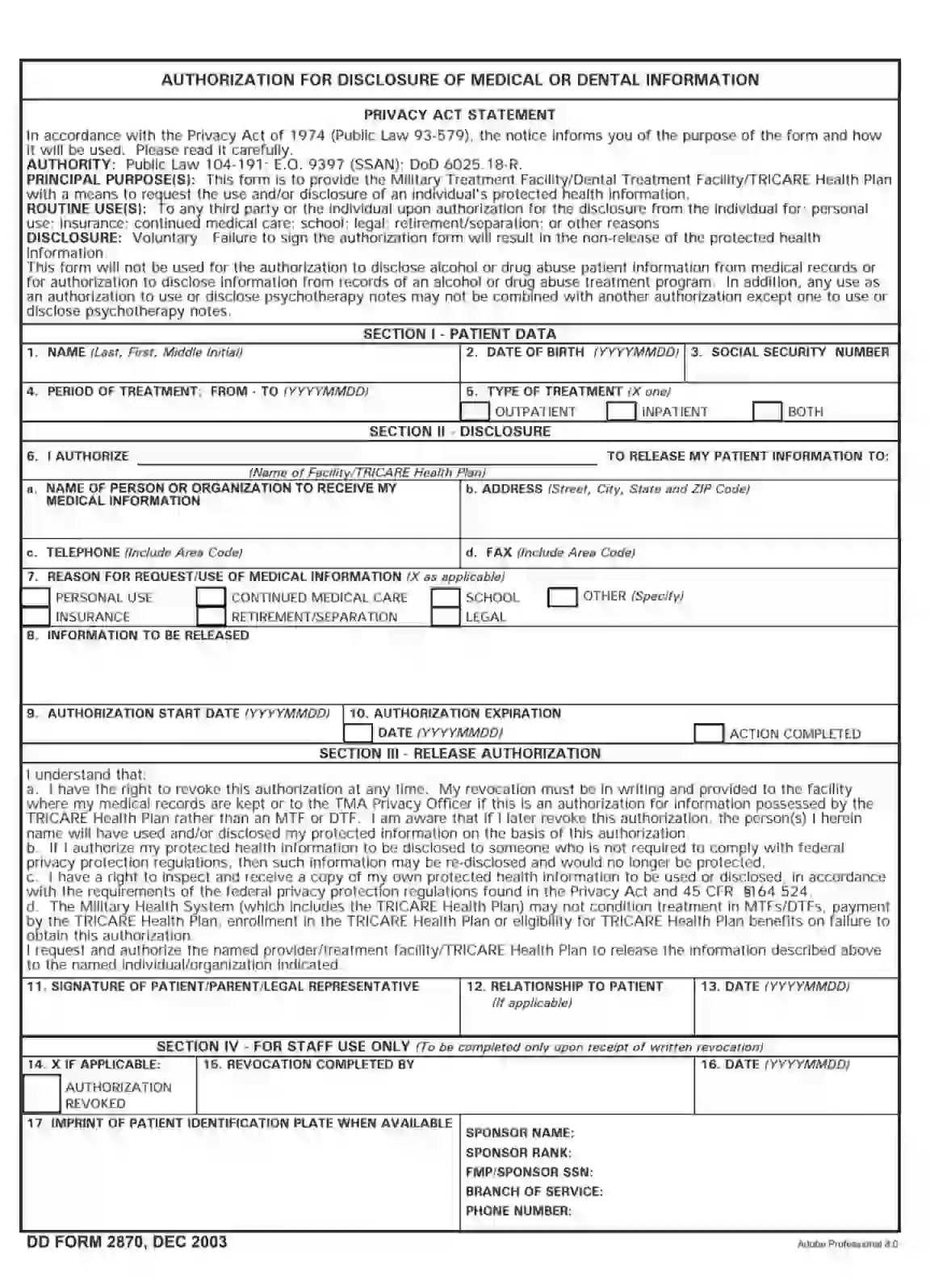
The paper is traditionally divided into three sections completed by the patient. The fourth part is filled out by the medical facility staff.
Each patient (declarant) needs to complete the three first sections providing valid personal info to the corresponding questions. You are welcome to generate the required PDF file by using our advanced software, print out, or type the template instantly.
Make sure to read the Privacy Act Statement at the top of the form to understand the purposes and limitations of the document clearly.
The first part consists of five blocks. The declarant should enter the expected data following the requirements:
Here, you should enter your first and last name, including the middle initial (if applicable).
By identifying the beginning and the expiration dates in a year-month-day format, the declarant allows the other person to have access to their private health records for the designated period.
“Outpatient” allows another person to get a disclosure of routine outpatient data. “Inpatient” reveals the info of someone who is admitted to the hospital with at least one overnight stay. If both variants apply, please, checkbox “Both.”
Some forms contain BHD access, which means that the patient allows another person to learn their psychiatric type info.

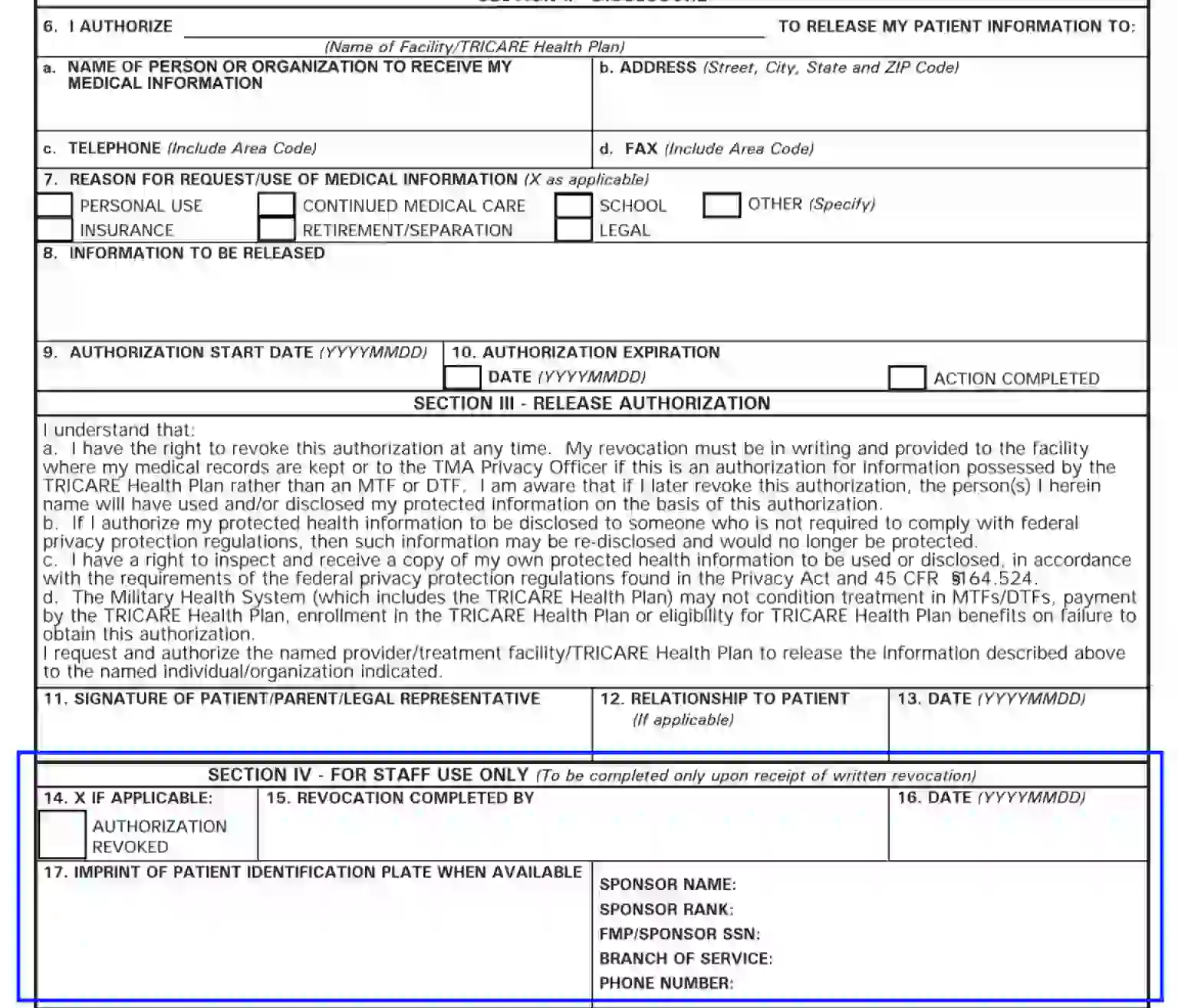
Section Two covers information revealing the patient’s trusted agent — a person who obtains access to the declarant’s medical records.
Enter the required name to allow your medical care service to disclose treatment data.

Here, the patient needs to enter the name of the trusted one (the agent) or the entity that gets access to the patient’s data and medical records.
Also, fill out the agent’s contact information, including the address (street, city, state, and ZIP), phone number, and fax.
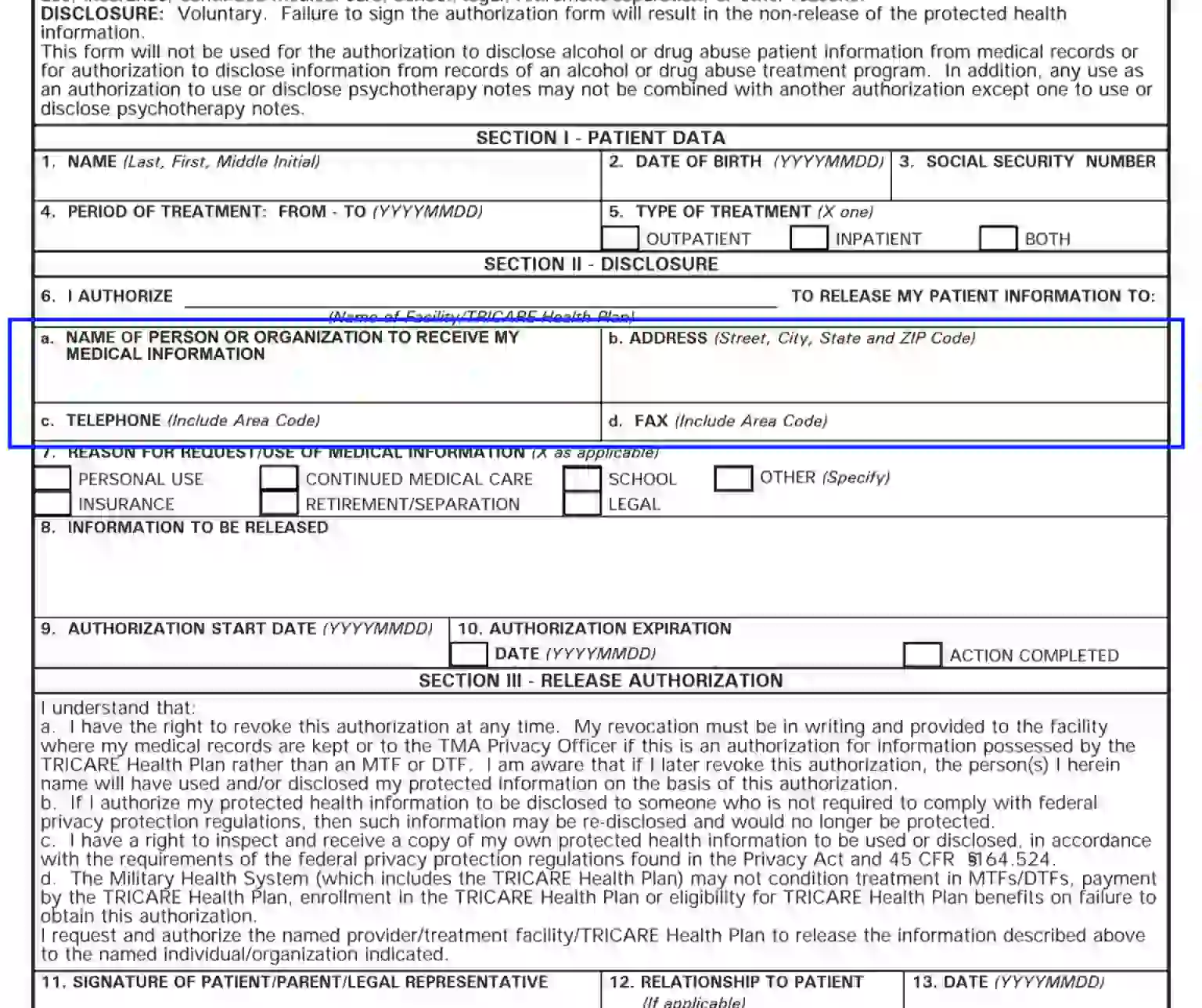
As the patient provides access to private records, they should give a reasonable ground in a written manner. This block demands that the declarant provides their reason by crossing the applicable alternative. If you decide to select the “Other” box, make sure to specify the reason shortly below.

Here, the patient should list the aspects regarding their treatment allowed to be released to the agent. Should you skip the block or leave it blank, the agent appointed in Unit 6 will get access to all your medical records.

In these parts, you need to outline the effective period, indicating both the start date and the expiration date. As a rule, DD Forms-2870 are effective for one year. However, the document will be disregarded without a selected expiration date.
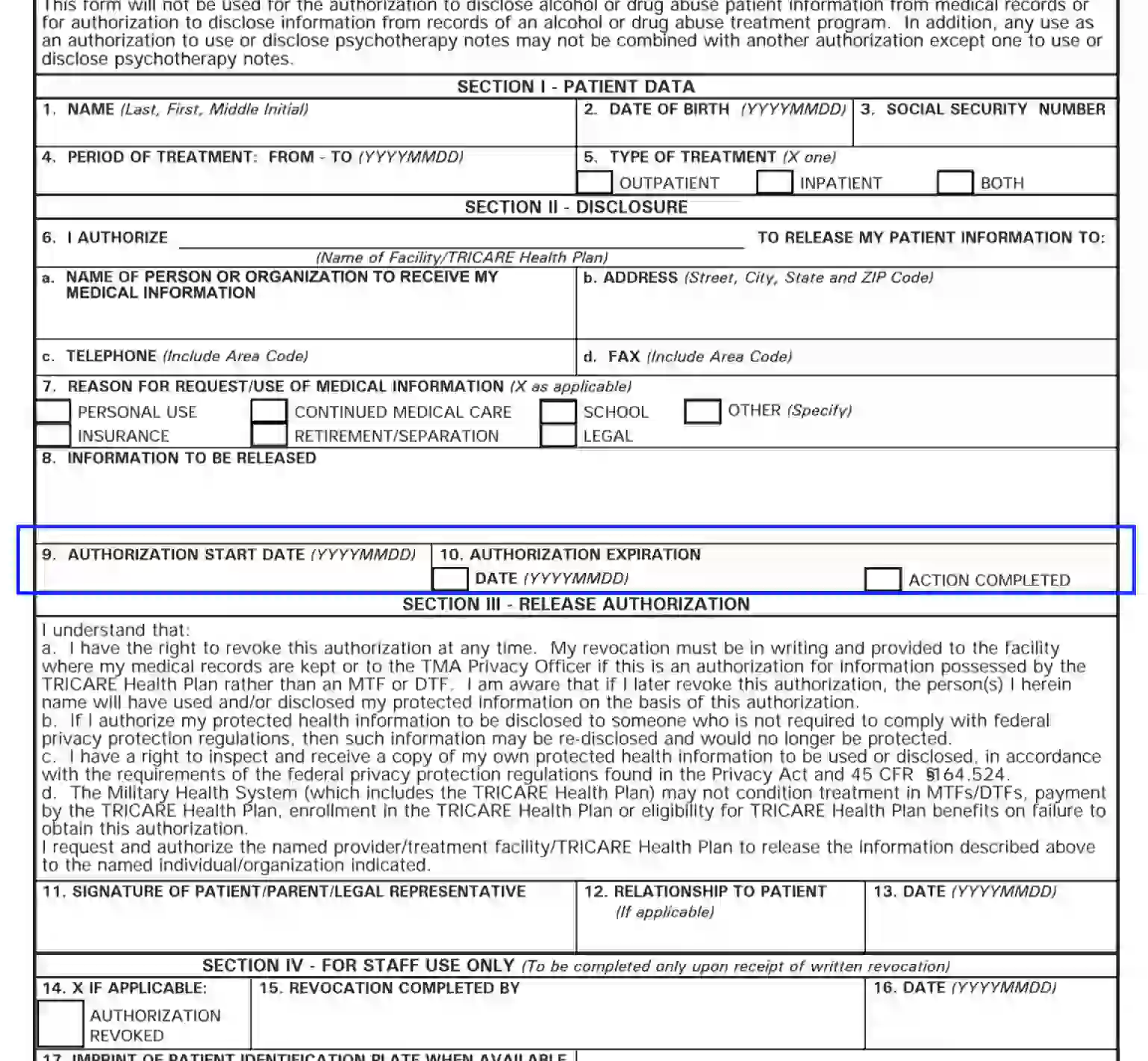
In Block 11, the patient, their parent, or the patient’s legal representative needs to give consent by appending the signature. In case the paper is authorized on the declarant’s behalf, the appointed guardian or representative should also indicate their relation to the patient.
Insert the current calendar date this document is created on.
This part is completed only by the facility representatives in case of revocation. The patient needs to provide the data indicated next to Block 17.