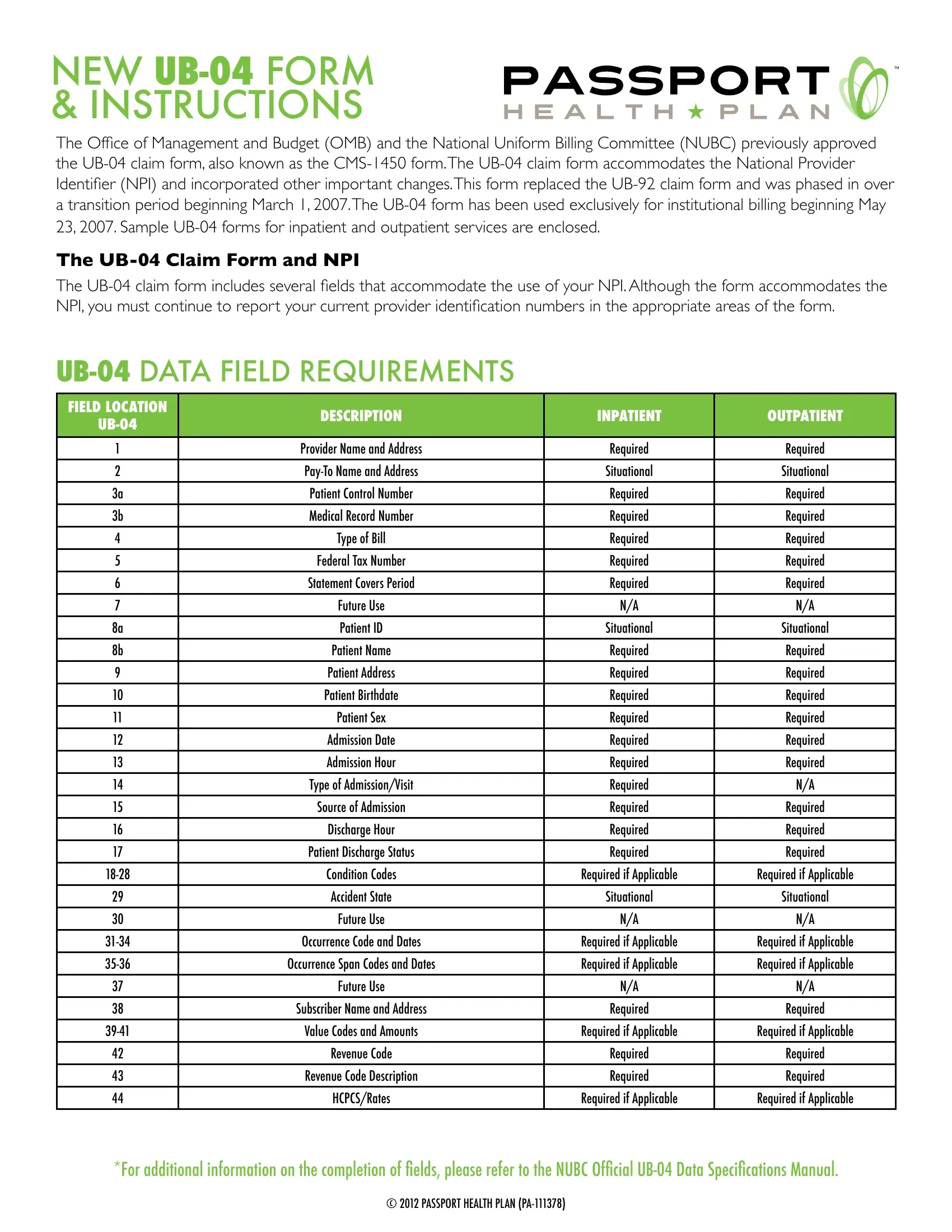
In the landscape of healthcare billing in the United States, the transition to the UB-04 claim form, also recognized as the CMS-1450, marks a pivotal evolution in institutional billing practices. Mandated by the Office of Management and Budget (OMB) and the National Uniform Billing Committee (NUBC), the adoption of this form, from March 1, 2007, reflects significant steps towards streamlining the process and accommodating the integration of the National Provider Identifier (NPI). The comprehensive UB-04 form caters to both inpatient and outpatient services, encapsulating a wide array of data requirements such as patient information, provider details, admissions data, and various codes essential for processing claims accurately. Rigorous in its design, the form includes fields for provider names, patient demographics, the type of bill, admission details, and an extensive list of condition and value codes, among others, to support the nuanced requirements of medical billing. The insistence on the usage of NPI alongside provider identification numbers underscores the form's role in the transition towards a more centralized and efficient electronic billing system. This change, exclusive since May 23, 2007, points towards a broader shift in healthcare administration, aiming to reduce complexities and improve the precision of claims processing. Moreover, the supplement of sample UB-04 forms and specific instructions for completion underlines the effort to guide healthcare providers through this detailed and critical documentation process, ensuring compliance and facilitation of timely reimbursements.
| Question | Answer |
|---|---|
| Form Name | 04 Form Printable |
| Form Length | 5 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 15 sec |
| Other names | aia product substitution request form, 04 form, ub 04 insurance form, printable ub 04 claim form |

new
The Ofice of Management and Budget (OMB) and the National Uniform Billing Committee (NUBC) previously approved the
THE
The
FIELD LOCATION |
DESCRIPTION |
INPATIENT |
OUTPATIENT |
|
|
|
|
||
|
|
|
|
|
1 |
Provider Name and Address |
Required |
Required |
|
2 |
Situational |
Situational |
||
3a |
Patient Control Number |
Required |
Required |
|
3b |
Medical Record Number |
Required |
Required |
|
|
|
|
|
|
4 |
Type of Bill |
Required |
Required |
|
|
|
|
|
|
5 |
Federal Tax Number |
Required |
Required |
|
6 |
Statement Covers Period |
Required |
Required |
|
7 |
Future Use |
N/A |
N/A |
|
8a |
Patient ID |
Situational |
Situational |
|
|
|
|
|
|
8b |
Patient Name |
Required |
Required |
|
|
|
|
|
|
9 |
Patient Address |
Required |
Required |
|
10 |
Patient Birthdate |
Required |
Required |
|
11 |
Patient Sex |
Required |
Required |
|
12 |
Admission Date |
Required |
Required |
|
|
|
|
|
|
13 |
Admission Hour |
Required |
Required |
|
|
|
|
|
|
14 |
Type of Admission/Visit |
Required |
N/A |
|
15 |
Source of Admission |
Required |
Required |
|
16 |
Discharge Hour |
Required |
Required |
|
17 |
Patient Discharge Status |
Required |
Required |
|
|
|
|
|
|
Condition Codes |
Required if Applicable |
Required if Applicable |
||
|
|
|
|
|
29 |
Accident State |
Situational |
Situational |
|
30 |
Future Use |
N/A |
N/A |
|
Occurrence Code and Dates |
Required if Applicable |
Required if Applicable |
||
Occurrence Span Codes and Dates |
Required if Applicable |
Required if Applicable |
||
|
|
|
|
|
37 |
Future Use |
N/A |
N/A |
|
|
|
|
|
|
38 |
Subscriber Name and Address |
Required |
Required |
|
Value Codes and Amounts |
Required if Applicable |
Required if Applicable |
||
42 |
Revenue Code |
Required |
Required |
|
43 |
Revenue Code Description |
Required |
Required |
|
|
|
|
|
|
44 |
HCPCS/Rates |
Required if Applicable |
Required if Applicable |
|
|
|
|
|
*For additional information on the completion of ields, please refer to the NUBC Oficial
© 2012 PASSPORT HEALTH PLAN

FIELD LOCATION |
DESCRIPTION |
INPATIENT |
OUTPATIENT |
|
|
|
|
||
|
|
|
|
|
45 |
Service Date |
N/A |
Required |
|
|
|
|
|
|
46 |
Units of Service |
Required |
Required |
|
|
|
|
|
|
47 |
Total Charges (By Rev. Code) |
Required |
Required |
|
48 |
Required if Applicable |
Required if Applicable |
||
49 |
Future Use |
N/A |
N/A |
|
50 |
Payer Identiication (Name) |
Required |
Required |
|
51 |
NPI |
Required |
Required |
|
|
|
|
|
|
52 |
Release of Info Certiication |
Required |
Required |
|
53 |
Assignment of Beneit Certiication |
Required |
Required |
|
54 |
Prior Payments |
Required if Applicable |
Required if Applicable |
|
55 |
Estimated Amount Due |
Required |
Required |
|
|
|
|
|
|
56 |
NPI |
Required |
Required |
|
|
|
|
|
|
57 |
Health Plan IDs |
Required |
Required |
|
58 |
Insured’s Name |
Required |
Required |
|
59 |
Patient’s Relation to the Insured |
Required |
Required |
|
60 |
Insured’s Unique ID |
Required |
Required |
|
61 |
Insured Group Name |
Situational |
Situational |
|
|
|
|
|
|
62 |
Insured Group Number |
Situational |
Situational |
|
63 |
Treatment Authorization Codes |
Required if Applicable |
Required if Applicable |
|
64 |
Document Control Number |
Situational |
Situational |
|
65 |
Employer Name |
Situational |
Situational |
|
|
|
|
|
|
66 |
Diagnosis/Procedure Code Qualiier |
Required |
Required |
|
67 |
Principal Diagnosis Code/Other Diagnosis Codes |
Required |
Required |
|
68 |
Future Use |
N/A |
N/A |
|
69 |
Admitting Diagnosis Code |
Required |
Required if Applicable |
|
70 |
Patient’s Reason for Visit Code |
Situational |
Situational |
|
71 |
PPS Code |
Situational |
Situational |
|
|
|
|
|
|
72 |
External Cause of Injury Code |
Situational |
Situational |
|
73 |
Future Use |
N/A |
N/A |
|
74 |
Principal Procedure Code/Date |
Required if Applicable |
Required if Applicable |
|
75 |
Future Use |
N/A |
N/A |
|
|
|
|
|
|
76 |
Attending Name/ |
Required |
Required |
|
77 |
Operating ID |
Situational |
Situational |
|
Other ID |
Situational |
Situational |
||
80 |
Remarks |
Situational |
Situational |
|
81 |
|
|
||
|
N/A |
N/A |
||
|
|
|
|
|
|
Situational |
Situational |
||
|
N/A |
N/A |
||
|
Situational |
Situational |
||
|
*B3 |
Required |
Required |
|
|
|
|
|
*For additional information on the completion of ields, please refer to the NUBC Oficial
© 2012 PASSPORT HEALTH PLAN
We would also like to remind you of the requirements for electronic transactions. As a reminder, Passport Health Plan strongly recommends the continued use of plan identiication numbers in addition to NPI.
837 I Data FielD RequiRements
LOOP ID
2000A
LOOP ID
2010AA
LOOP ID
2010AA
====================== 837 I ====================== BILLING TAXONOMY LOOP ======================
Loop Name |
|
Segment Name |
|
PRV01 Qualiier |
PRV02 Qualiier |
PRV03 Value |
||
|
PRV |
|
BI |
ZZ |
= Taxonomy |
|||
|
|
PT |
||||||
|
|
|
|
|
|
|
||
====================== 837 I ====================== BILLING PROVIDER LOOP ====================== |
|
|
||||||
|
|
|||||||
|
|
|
|
|
|
|
|
|
Loop Name |
|
Segment Name |
|
NM101 Qualiier |
NM108 Qualiier |
NM109 Value |
||
|
|
|
|
|
|
24 |
= TAX ID |
|
Billing Provider |
|
NM1 |
|
85 |
|
34 |
= SSN |
|
|
|
|
|
|
|
XX |
= NPI |
|
Loop Name |
|
Segment Name |
|
REF01 Qualiier |
|
|
REF02 Value |
|
|
|
|
|
|
||||
|
|
|
|
|
||||
|
|
|
|
SY |
|
|
= SSN |
|
Billing Provider Secondary Identiication |
|
REF |
|
EI |
|
|
= TAX ID |
|
|
|
|
|
1D |
|
|
= MAID |
|
|
|
|
|
|
|
|
|
|
LOOP ID
2010AB
LOOP ID
2010AB
LOOP ID
2310A
LOOP ID
2310A
LOOP ID
2310E
LOOP ID
2310E
====================== 837 I ====================== PAY TO PROVIDER LOOP ======================
Loop Name |
|
Segment Name |
|
NM101 Qualiier |
|
NM108 Qualiier |
|
NM109 Value |
||
|
|
|
|
|
|
|
24 |
|
= TAX ID |
|
|
NM1 |
|
87 |
|
|
34 |
|
= SSN |
||
|
|
|
|
|
|
|
XX |
|
= NPI |
|
Loop Name |
|
Segment Name |
|
REF01 Qualiier |
|
|
|
|
REF02 Value |
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
||||
|
|
|
|
SY |
|
|
|
|
|
|
|
REF |
|
EI |
|
|
|
|
|
|
|
|
|
|
|
1D |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
====================== 837 I ====================== ATTENDING PROVIDER LOOP ====================== |
|
|
|
|||||||
|
|
|
||||||||
Loop Name |
|
Segment Name |
|
NM101 Qualiier |
|
NM108 Qualiier |
|
NM109 Value |
||
|
|
|
|
|||||||
|
|
|
|
|
|
|
24 |
|
= TAX ID |
|
Attending Physician |
|
NM1 |
|
82 |
|
|
34 |
|
= SSN |
|
|
|
|
|
|
|
|
XX |
|
= NPI |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
Loop Name |
|
Segment Name |
|
REF01 Qualiier |
|
|
|
|
REF02 Value |
|
Attending Physician Secondary Identiication |
|
REF |
|
N5 |
|
|
|
|
= Facets ID |
|
====================== 837 I ====================== SERVICE FACILITY LOOP ====================== |
|
|
|
|||||||
|
|
|
||||||||
Loop Name |
|
Segment Name |
|
NM101 Qualiier |
|
NM108 Qualiier |
|
NM109 Value |
||
|
|
|
|
|||||||
|
|
|
|
|
|
|
24 |
|
= TAX ID |
|
Service Facility Location |
|
NM1 |
|
82 |
|
|
34 |
|
= SSN |
|
|
|
|
|
|
|
|
XX |
|
= NPI |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
||
Loop Name |
|
Segment Name |
|
REF01 Qualiier |
|
|
|
|
REF02 Value |
|
Service Facility Location Secondary Identiication |
|
REF |
|
N5 |
|
|
|
|
= Facets ID |
|
|
|
|
|
|
|
|
|
|
|
|
Please let us know if you have any questions regarding these instructions. In addition, if you have any questions regarding the NPI, the application process, or reporting your NPIs to us, please contact your Provider Relations representative.
© 2012 PASSPORT HEALTH PLAN